

Multicenter Evaluation of the QIAstat-Dx and the BioFire Multiplex Panel Tests for the Detection of Respiratory Pathogens
- PMID: 39711468
- PMCID: PMC11664495
- DOI: 10.1002/jmv.70129
Multicenter Evaluation of the QIAstat-Dx and the BioFire Multiplex Panel Tests for the Detection of Respiratory Pathogens
Abstract
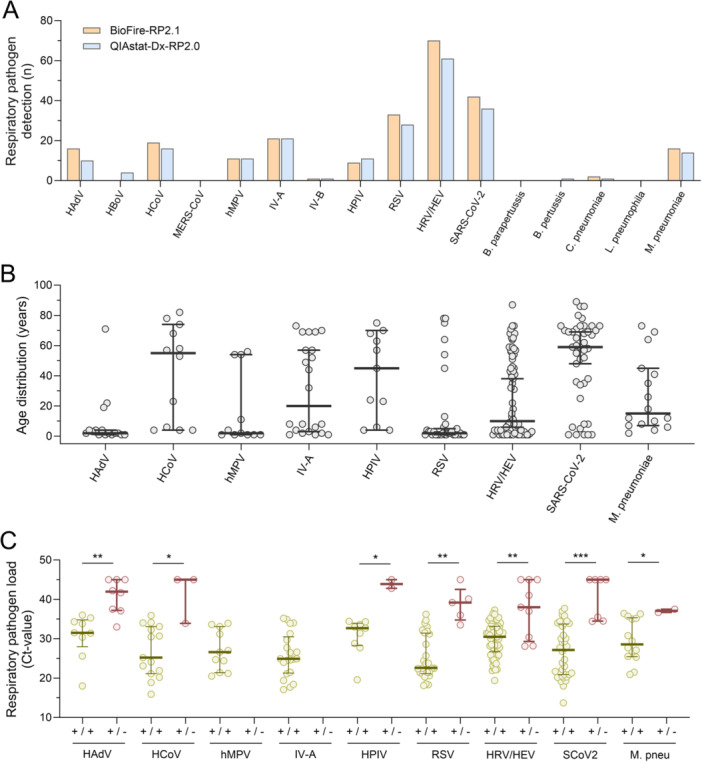
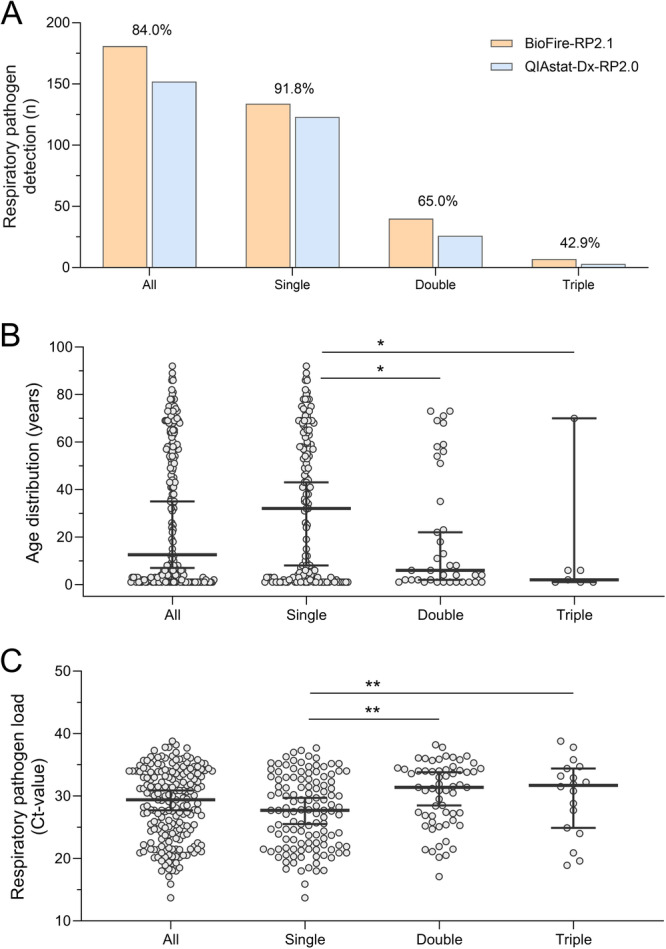
Syndromic multiplex panel testing enables simultaneous detection of multiple respiratory pathogens, but limited data is available on the comparative diagnostic performance of different testing systems. In this multicenter prospective study, we aimed to compare the QIAstat-Dx Respiratory Panel 2.0 (QIAstat-Dx-RP2.0) with the widely used BioFire-RP2.1, using 269 respiratory clinical specimens. Concordant test results were obtained in 232 (86.3%) cases. Discordant test results included 33 BioFire-RP2.1(+)/QIAstat-Dx-RP2.0(-) and 4 BioFire-RP2.1(-)/QIAstat-Dx-RP2.0(+) results. Discordant samples showed significantly lower pathogen loads than concordant ones (p < 0.01). Overall, the QIAstat-Dx-RP2.0 showed an analytical sensitivity of 50%-100% depending on the respiratory target, with an analytical specificity ≥ 99.0%. Most significant differences were found for the detection of adenovirus, human coronaviruses, respiratory syncytial virus, human rhinovirus/enterovirus and SARS-CoV-2 (kappa-score: 0.67-0.91). Co-detections of respiratory pathogens were identified in 47 cases by BioFire-RP2.1 and 29 by QIAstat-Dx-RP2.0. Agreement rates between the two multiplex panel tests decreased from 91.8% for single pathogen detections to 65.0% and 42.9% for co-detecting two and three pathogens, respectively. Pathogen loads were significantly lower in co-detections compared to single pathogen detections (p < 0.01), potentially explaining the lower detection rates with the QIAstat-Dx-RP2.0 in cases of multiple pathogens. In conclusion, our prospective multicenter evaluation showed good diagnostic performance of the QIAstat-Dx-RP2.0 assay, but lower detection rates for some respiratory targets compared to BioFire-RP2.1. As QIAstat-Dx-RP2.0 offers advantages in handling, noise emission, cost effectiveness, and provides semi-quantitative results compared to BioFire-RP2.1 an updated version with enhanced analytical sensitivity would be a viable alternative syndromic testing system for detecting respiratory pathogens.
Keywords: BioFire; QIAstat‐Dx; RSV; SARS‐CoV‐2; adenovirus; influenza; respiratory pathogen; respiratory tract infection; rhinovirus/enterovirus; syndromic multiplex panel testing.
© 2024 The Author(s). Journal of Medical Virology published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Ferkol T. and Schraufnagel D., “The Global Burden of Respiratory Disease,” Annals of the American Thoracic Society 11, no. 3 (2014): 404–406. - PubMed
-
- Gonzales R., Malone D. C., Maselli J. H., and Sande M. A., “Excessive Antibiotic Use for Acute Respiratory Infections in the United States,” Clinical Infectious Diseases 33, no. 6 (2001): 757–762. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
