

Plasma acute phase proteins as potential predictors of intra-amniotic inflammation and infection in preterm premature rupture of membranes
- PMID: 39711480
- PMCID: PMC11664557
- DOI: 10.1177/17534259241306237
Plasma acute phase proteins as potential predictors of intra-amniotic inflammation and infection in preterm premature rupture of membranes
Abstract
Background: We aimed to investigate the potential of altered levels of various acute phase proteins (APPs) in the plasma, either used alone or in combination with ultrasound-, clinical-, and conventional blood-based tests, for predicting the risk of intra-amniotic inflammation (IAI), microbial invasion of the amniotic cavity (MIAC), histologic chorioamnionitis (HCA), and funisitis in women with preterm premature rupture of membranes (PPROM).
Methods: A total of 195 consecutive pregnancies involving singleton women with PPROM (at 23 + 0-34 + 0 weeks) who underwent amniocentesis and from whom plasma samples were obtained at amniocentesis were retrospectively included in this study. Amniotic fluid (AF) was cultured to assess the MIAC and analyzed for interleukin (IL)-6 levels to define IAI (AF IL-6 level of ≥2.6 ng/mL). The plasma concentrations of hepcidin, mannose-binding lectin (MBL), pentraxin-2, retinol-binding protein 4 (RBP4), serum amyloid A1 (SAA1), and serpin A1 were determined using ELISA. Ultrasonographic cervical length (CL), neutrophil-to-lymphocyte ratio (NLR), and C-reactive protein levels were measured. IAI/MIAC was defined as IAI, MIAC, or both.
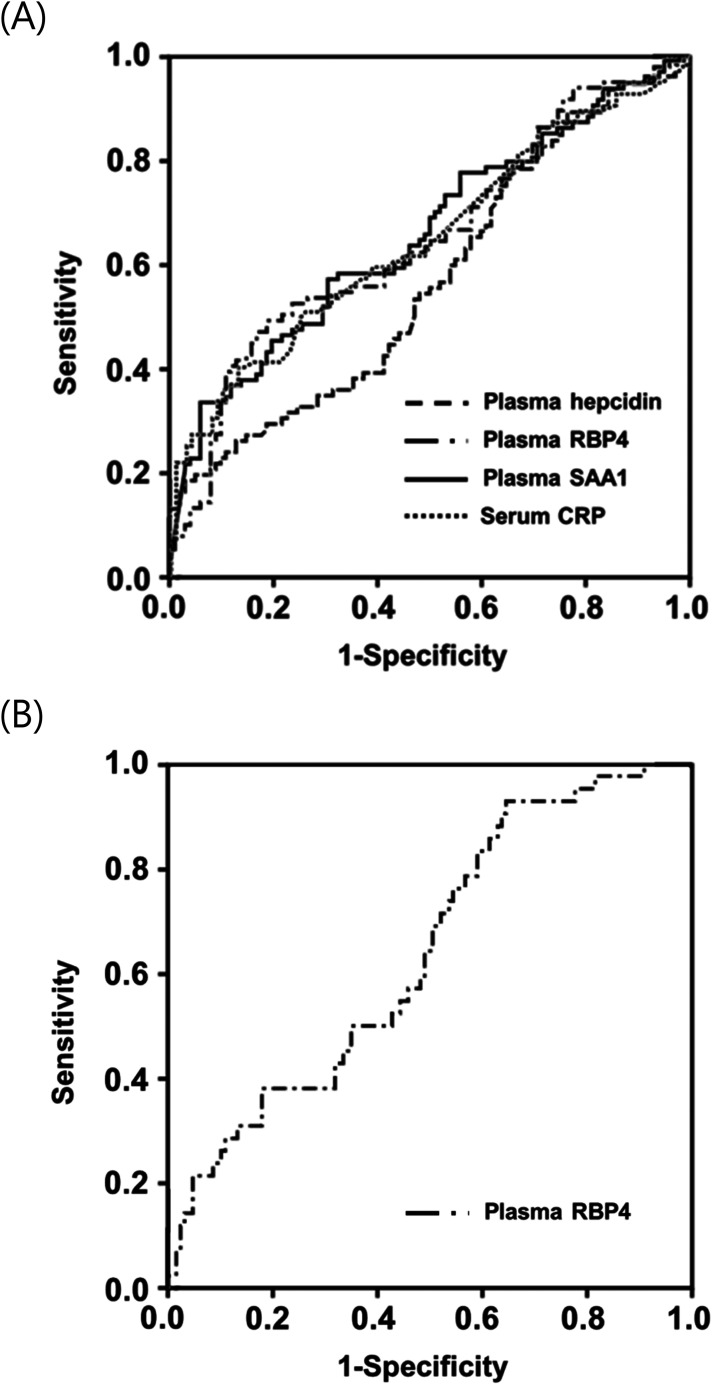
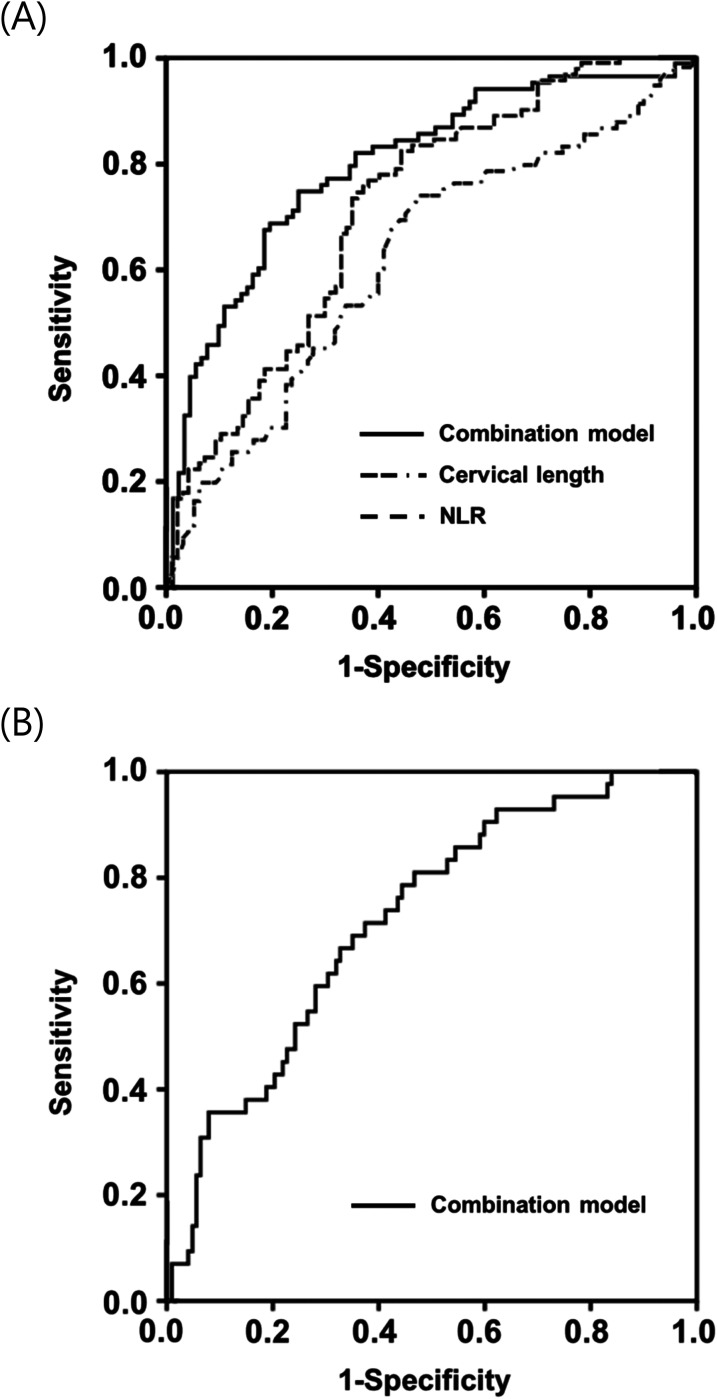
Results: Multivariate logistic regression analyses showed the following: (1) elevated plasma levels of hepcidin and SAA1 and decreased levels of RBP4 in the plasma were independently associated with IAI/MIAC and (2) decreased plasma RBP4 levels were independently associated with funisitis; however, (3) none of the plasma APPs investigated were associated with acute HCA when adjusted for baseline covariates. Using stepwise regression analysis, noninvasive prediction models comprising plasma RBP4 levels, CL, NLR, and gestational age at sampling were proposed, which provided a good prediction of IAI/MIAC and funisitis (area under the curve: 0.80 and 0.72, respectively).
Conclusions: Hepcidin, RBP4, and SAA1 were identified as potential APP biomarkers in the plasma predictive of IAI/MIAC or funisitis in patients with PPROM. In particular, combination of these APP biomarkers with ultrasound-, clinical-, and conventional blood-based markers can significantly support the diagnosis of IAI/MIAC and funisitis.
Keywords: Acute phase proteins; funisitis; intra-amniotic inflammation; microbial invasion of the amniotic cavity; plasma; prediction model; preterm premature rupture of membranes.
Conflict of interest statement
Declaration of conflicting interestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Sae-Lin P, Wanitpongpan P. Incidence and risk factors of preterm premature rupture of membranes in singleton pregnancies at Siriraj Hospital. J Obstet Gynaecol Res 2019; 45: 573–577. - PubMed
-
- Menon R, Fortunato SJ. Infection and the role of inflammation in preterm premature rupture of the membranes. Best Pract Res Clin Obstet Gynaecol 2007; 21: 467–478. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
