

This is a preprint.
Towards pandemic preparedness: ability to estimate high-resolution social contact patterns from longitudinal surveys
- PMID: 39711531
- PMCID: PMC11661306
- DOI: 10.21203/rs.3.rs-5182601/v1
Towards pandemic preparedness: ability to estimate high-resolution social contact patterns from longitudinal surveys
Update in
-
Addressing survey fatigue bias in longitudinal social contact studies to improve pandemic preparedness.Sci Rep. 2025 May 23;15(1):17935. doi: 10.1038/s41598-025-02235-0. Sci Rep. 2025. PMID: 40410335 Free PMC article.
Abstract
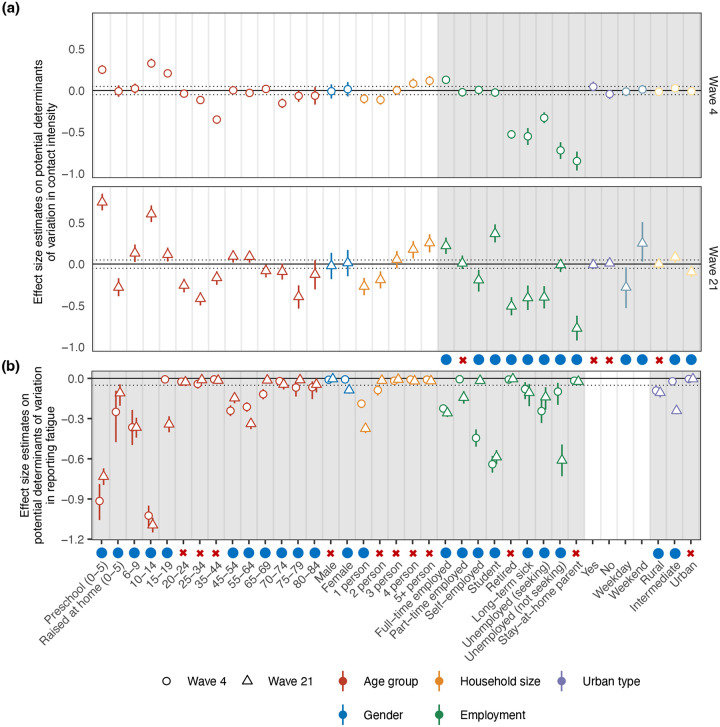
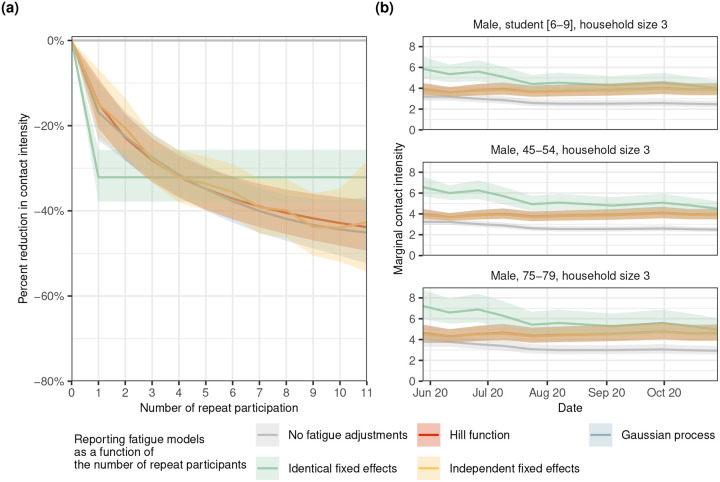
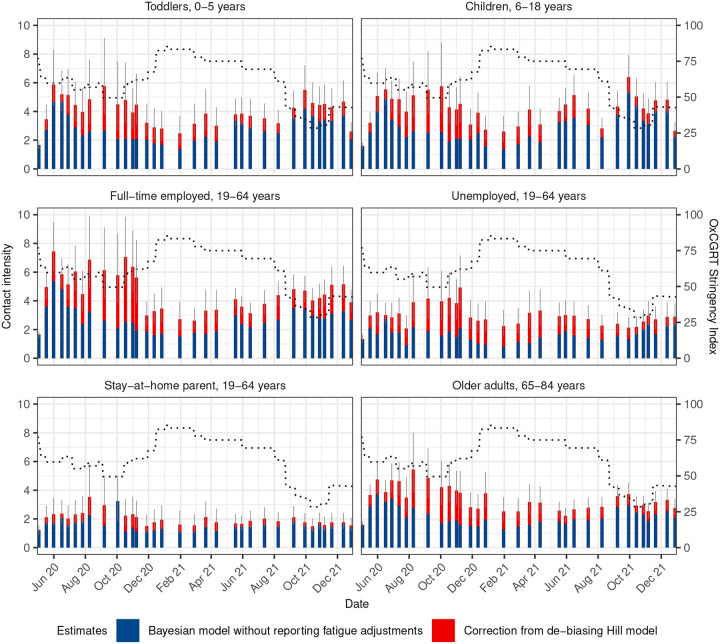
Social contact surveys are an important tool to assess infection risks within populations, and the effect of non-pharmaceutical interventions on social behaviour during disease outbreaks, epidemics, and pandemics. Numerous longitudinal social contact surveys were conducted during the COVID-19 era, however data analysis is plagued by reporting fatigue, a phenomenon whereby the average number of social contacts reported declines with the number of repeat participations and as participants' engagement decreases over time. Using data from the German COVIMOD Study between April 2020 to December 2021, we demonstrate that reporting fatigue varied considerably by sociodemographic factors and was consistently strongest among parents reporting children contacts (parental proxy reporting), students, middle-aged individuals, those in full-time employment and those self-employed. We find further that, when using data from first-time participants as gold standard, statistical models incorporating a simple logistic function to control for reporting fatigue were associated with substantially improved estimation accuracy relative to models with no reporting fatigue adjustments, and that no cap on the number of repeat participations was required. These results indicate that existing longitudinal contact survey data can be meaningfully interpreted under an easy-to-implement statistical approach adressing reporting fatigue confounding, and that longitudinal designs including repeat participants are a viable option for future social contact survey designs.
Conflict of interest statement
Additional Declarations: No competing interests reported. Competing interests The authors declare no competing interests.
Figures


References
-
- James S. L. et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet 392, 1789–1858, DOI: 10.1016/S0140-6736(18)32279-7 (2018). Publisher: Elsevier. - DOI - PMC - PubMed
-
- Roth G. A. et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet 392, 1736–1788, DOI: 10.1016/S0140-6736(18)32203-7 (2018). Publisher: Elsevier. - DOI - PMC - PubMed
-
- Killingley B. & Nguyen-Van-Tam J. Routes of influenza transmission. Influ. Other Respir. Viruses 7, 42–51, DOI: 10.1111/irv.12080 (2013). _eprint: https://onlinelibrary.wiley.com/doi/pdf/10.1111/irv.12080. - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
