

Enhancing Perioperative Outcomes of Pancreatic Surgery with Wearable Augmented Reality Assistance System: A Matched-Pair Analysis
- PMID: 39711676
- PMCID: PMC11661739
- DOI: 10.1097/AS9.0000000000000516
Enhancing Perioperative Outcomes of Pancreatic Surgery with Wearable Augmented Reality Assistance System: A Matched-Pair Analysis
Abstract
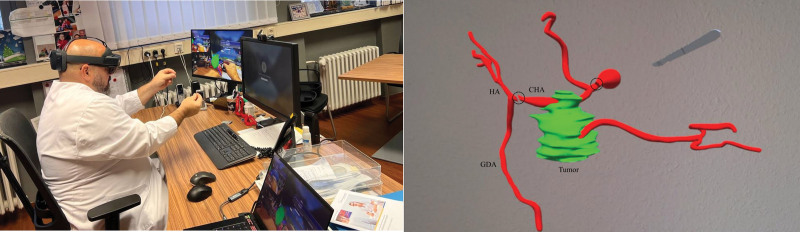
Objective: The present study aimed to evaluate the safety of the first wearable augmented reality assistance system (ARAS) specifically designed for pancreatic surgery and its impact on perioperative outcomes.
Background: Pancreatic surgery remains highly complex and is associated with a high rate of perioperative complications. ARAS, as an intraoperative assistance system, has the potential to reduce these complications.
Methods: This prospective, single-center study included 20 patients who underwent pancreatic surgery using ARAS. These patients were matched in a 1:3 ratio with 60 patients from our retrospective data who underwent standard pancreatic resection. Matching variables were selected based on factors associated with poor intraoperative outcomes.
Results: A higher proportion of patients in the ARAS group were diagnosed with borderline resectable pancreatic cancer and received neoadjuvant chemotherapy (20.0% vs 6.7%, P = 0.085). Additionally, more patients in the ARAS group required arterial resection compared with the control group (15.0% vs 0.0%, P = 0.002). Nevertheless, the ARAS group had a significantly shorter operative time (246 vs 299 minutes, P = 0.004) and required significantly fewer intraoperative blood transfusions (0.0 ± 0.0 vs 0.5 ± 1.4 units, P = 0.014). None of the patients in the ARAS group had positive resection margins (0.0% vs 20.0%, P = 0.045). Furthermore, patients in the ARAS group experienced a significantly shorter hospital stay (13.8 ± 6.6 vs 17.9 ± 8.2 days, P = 0.046).
Conclusions: ARAS is a safe and effective assistance system for pancreatic surgery, offering superior perioperative outcomes compared with standard procedures.
Keywords: augmented reality; navigation system; pancreatectomy; surgical planning; wearable devices.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Disclosure: The authors declare that they have nothing to disclose.
Figures


References
-
- Klotz R, Hackert T, Heger P, et al. . The TRIANGLE operation for pancreatic head and body cancers: early postoperative outcomes. HPB. 2022;24:332–341. - PubMed
-
- Hackert T, Strobel O, Michalski CW, et al. . The TRIANGLE operation–radical surgery after neoadjuvant treatment for advanced pancreatic cancer: a single arm observational study. HPB. 2017;19:1001–1007. - PubMed
-
- Heestand GM, Murphy JD, Lowy AM. Approach to patients with pancreatic cancer without detectable metastases. J Clin Oncol. 2015;33:1770–1778. - PubMed
-
- Sánchez-Velázquez P, Muller X, Malleo G, et al. . Benchmarks in pancreatic surgery: a novel tool for unbiased outcome comparisons. Ann Surg. 2019;270:211–218. - PubMed
LinkOut - more resources
Full Text Sources
