

Operationalizing the New Global Definition of ARDS: A Retrospective Cohort Study From South Africa
- PMID: 39711978
- PMCID: PMC11661813
- DOI: 10.1016/j.chstcc.2024.100103
Operationalizing the New Global Definition of ARDS: A Retrospective Cohort Study From South Africa
Abstract
Background: A proposed new global definition of ARDS seeks to update the Berlin definition and account for nonintubated ARDS and ARDS diagnoses in resource-variable settings.
Research question: How do ARDS epidemiologic characteristics change with operationalizing the new global definition of ARDS in a resource-limited setting?
Study design and methods: We performed a real-use retrospective cohort study among adult patients meeting criteria for the Berlin definition of ARDS or the global definition of ARDS at ICU admission in two public hospitals in the KwaZulu-Natal Department of Health, South Africa, from January 2017 through June 2022.
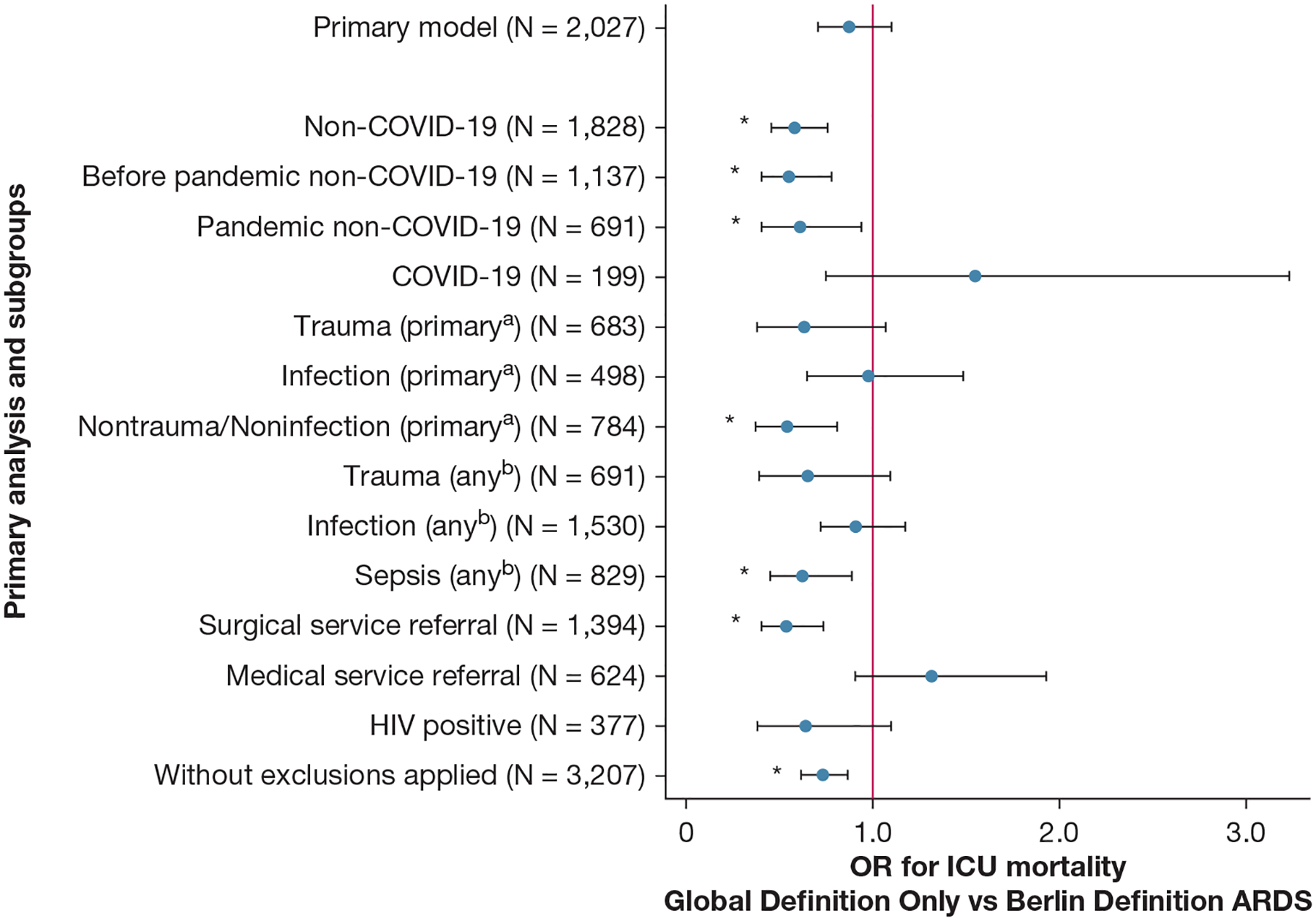
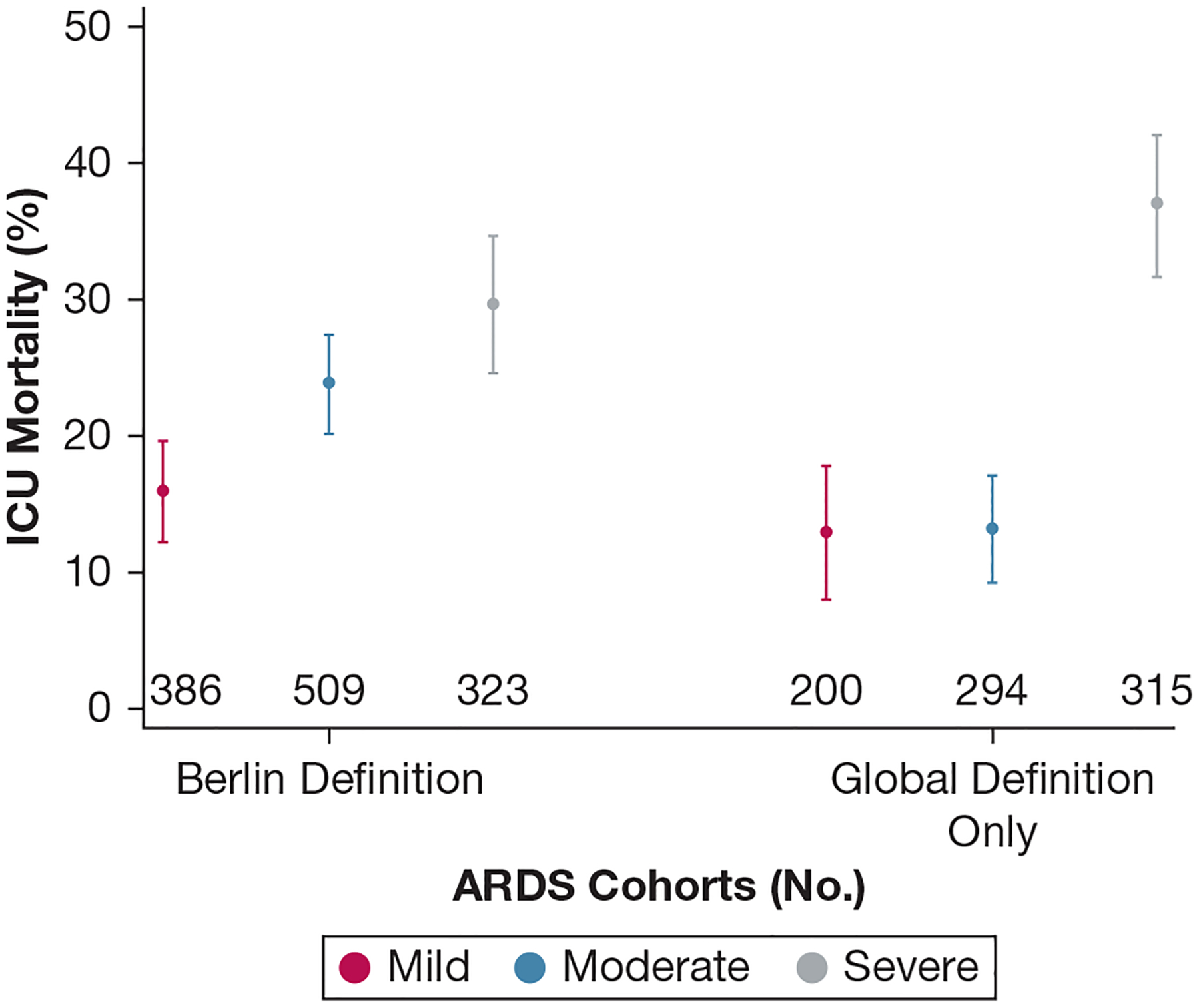
Results: Among 5,760 adults (aged ≥ 18 years) admitted to the ICU, 2,027 patients (35.2%) met at least one ARDS definition, including 1,218 patients meeting the Berlin definition of ARDS (60.1% of all ARDS diagnoses) and 809 new diagnoses of the global definition of ARDS that were not captured by the Berlin definition alone (39.9% of all ARDS diagnoses and 14.0% of all ICU admissions). After adjustment for hospital-level factors, patients who met only the global definition of ARDS criteria (ie, who would not have been captured by the Berlin definition) showed no statistically significant ICU mortality difference vs patients with ARDS according to the Berlin definition (21.7% [95% CI, 18.9%-24.4%] vs 23.8% [95% CI, 21.5%-26.2%]; OR, 0.88 [95% CI, 0.70-1.10]; P = .25). In prespecified exploratory subgroup analyses, patients without COVID-19 who met only the criteria for the global definition of ARDS showed reduced ICU mortality (14.2% [95% CI, 11.6%-16.9%] vs 22.2% [95% CI, 19.8%-24.6%]; OR, 0.58 [95% CI, 0.45-0.75]; P < .0005) compared with patients without COVID-19 who met the Berlin definition for ARDS.
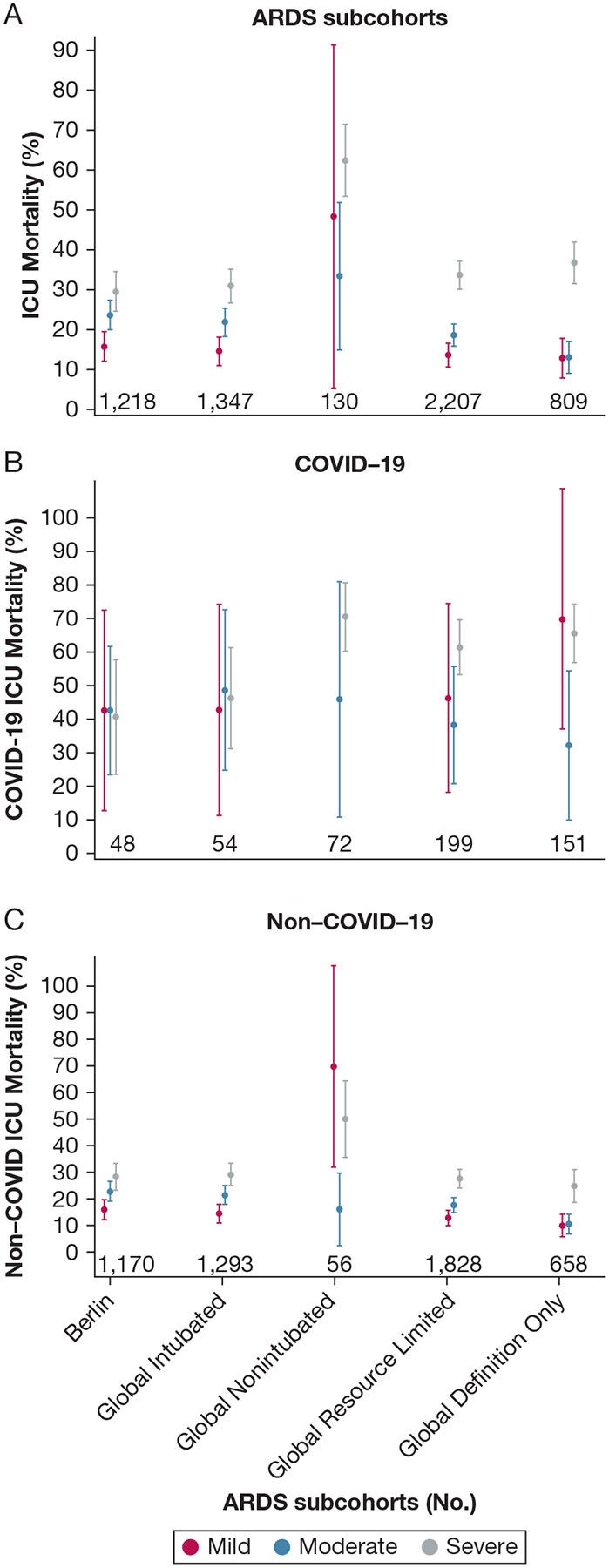
Interpretation: The new global definition of ARDS captures a significant proportion of patients who would not have been included by the Berlin definition alone. These additional patients with ARDS may have heterogenous patterns of outcomes among diagnostic subgroups, including by COVID-19 status, compared with patients with ARDS according to the Berlin definition.
Keywords: ARDS; COVID-19; global health; low-income and middle-income countries; resource-limited settings.
Figures
References
-
- Force ADT, Ranieri VM, Rubenfeld GD, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–2533. - PubMed
-
- Kwizera A, Dunser MW. A global perspective on acute respiratory distress syndrome and the truth about hypoxia in resource-limited settings. Am J Respir Crit Care Med. 2016;193(1):5–7. - PubMed
-
- Riviello ED, Kiviri W, Twagirumugabe T, et al. Hospital incidence and outcomes of the acute respiratory distress syndrome using the Kigali modification of the Berlin definition. Am J Respir Crit Care Med. 2016;193(1):52–59. - PubMed
-
- Bellani G, Laffey JG, Pham T, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788–800. - PubMed
-
- Santa Cruz R, Matesa A, Gomez A, et al. Mortality due to acute respiratory distress syndrome in Latin America. Crit Care Med. 2024;52(8):1275–1284. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous