

Double gas transfer factors (DLCO-DLNO) at rest in patients with congenital heart diseases correlates with their ventilatory response during maximal exercise
- PMID: 39712052
- PMCID: PMC11657256
- DOI: 10.1016/j.ijcchd.2022.100346
Double gas transfer factors (DLCO-DLNO) at rest in patients with congenital heart diseases correlates with their ventilatory response during maximal exercise
Abstract
Aim: Exercise capacity is altered in congenital heart diseases (CHD) with potentially impaired pulmonary perfusion adaptation during exercise, such as in single ventricle or in significant pulmonary regurgitation. This study aimed to evaluate the value of double gas transfer factor analysis, at rest in conjunction with postural manoeuvres, to explore the various components of pulmonary gas transfer and its association with exercise capacity.
Methods: A total of 40 subjects (24 CHD, 16 controls) underwent a combined measurement of lung diffusing capacity for carbon monoxide and nitric oxide (DLCO-DLNO) to determine pulmonary membrane diffusion (Dm) and Vcap, in sitting then supine position. CHD patients performed a maximal cardiopulmonary exercise test.
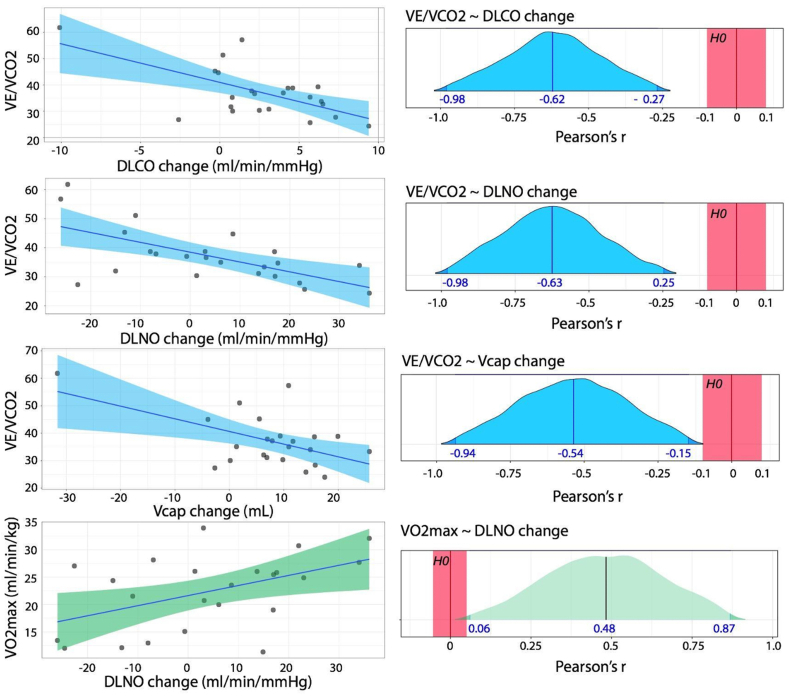
Results: Compared to normal controls, the CHD group's DLNO, DLCO, Vcap, and alveolar volume (AV) at rest, in the sitting position were depressed, whereas the DLCO/AV and DLNO/AV were similar. The magnitude of Dm and Vcap adaptation induced by postural change was similar in both groups, indicating a preserved pulmonary capillary recruitment capacity in CHD. In the CHD group, at rest, for each ml of postural-induced increase in Vcap we observed during exercise a VE/VCO2 slope decrease of 0.46 (95% CI[0.83; 0.098]), indicating a better ventilatory response to exercise.
Conclusion: CHD patients with impaired pulmonary circulation have a reduced Dm and Vcap mainly due to decreased pulmonary volume but maintain a normal capacity to adapt these parameters through a simple recruitment manoeuver. Vcap adaptation evaluated at rest predicts the level of ventilatory efficiency during exercise, which represents a main limiting factor in these CHD patients.
Keywords: Combined measurement of lung diffusion; Congenital heart disease; Exercise capacity; Pulmonary circulation; Pulmonary regurgitation; Single ventricle.
© 2022 The Authors.
Conflict of interest statement
The authors have no competing interests to declare.
Figures

Similar articles
-
Lung diffusion capacity for nitric oxide and carbon monoxide is impaired similarly following short-term graded exercise.Nitric Oxide. 2005 Feb;12(1):31-8. doi: 10.1016/j.niox.2004.11.002. Epub 2004 Dec 22. Nitric Oxide. 2005. PMID: 15631945 Clinical Trial.
-
Pulmonary membrane diffusing capacity and capillary blood volume measured during exercise from nitric oxide uptake.Chest. 2001 Dec;120(6):1850-6. doi: 10.1378/chest.120.6.1850. Chest. 2001. PMID: 11742912
-
Pulmonary diffusing capacity to nitric oxide and carbon monoxide during exercise and in the supine position: a test-retest reliability study.Exp Physiol. 2023 Feb;108(2):307-317. doi: 10.1113/EP090883. Epub 2023 Jan 9. Exp Physiol. 2023. PMID: 36621806 Free PMC article. Clinical Trial.
-
The DLNO/DLCO ratio: Physiological significance and clinical implications.Respir Physiol Neurobiol. 2017 Jul;241:17-22. doi: 10.1016/j.resp.2017.01.002. Epub 2017 Jan 11. Respir Physiol Neurobiol. 2017. PMID: 28088638 Review.
-
Simultaneous measurement of pulmonary diffusing capacity for carbon monoxide and nitric oxide.Respir Investig. 2018 Mar;56(2):100-110. doi: 10.1016/j.resinv.2017.12.006. Epub 2018 Feb 2. Respir Investig. 2018. PMID: 29548647 Review.
Cited by
-
Cardiac Fatigue in Male Athletes with Exercise-Induced Pulmonary Impairments After a Very Long-Distance Triathlon.Sports Med. 2025 Mar;55(3):739-751. doi: 10.1007/s40279-024-02128-8. Epub 2024 Oct 16. Sports Med. 2025. PMID: 39414722 Free PMC article.
References
LinkOut - more resources
Full Text Sources
