

What can we learn from systematic segmental analysis of fetal heart by postmortem micro-CT: Is it time to change approach?
- PMID: 39712275
- PMCID: PMC11657735
- DOI: 10.1016/j.ijcchd.2021.100308
What can we learn from systematic segmental analysis of fetal heart by postmortem micro-CT: Is it time to change approach?
Abstract
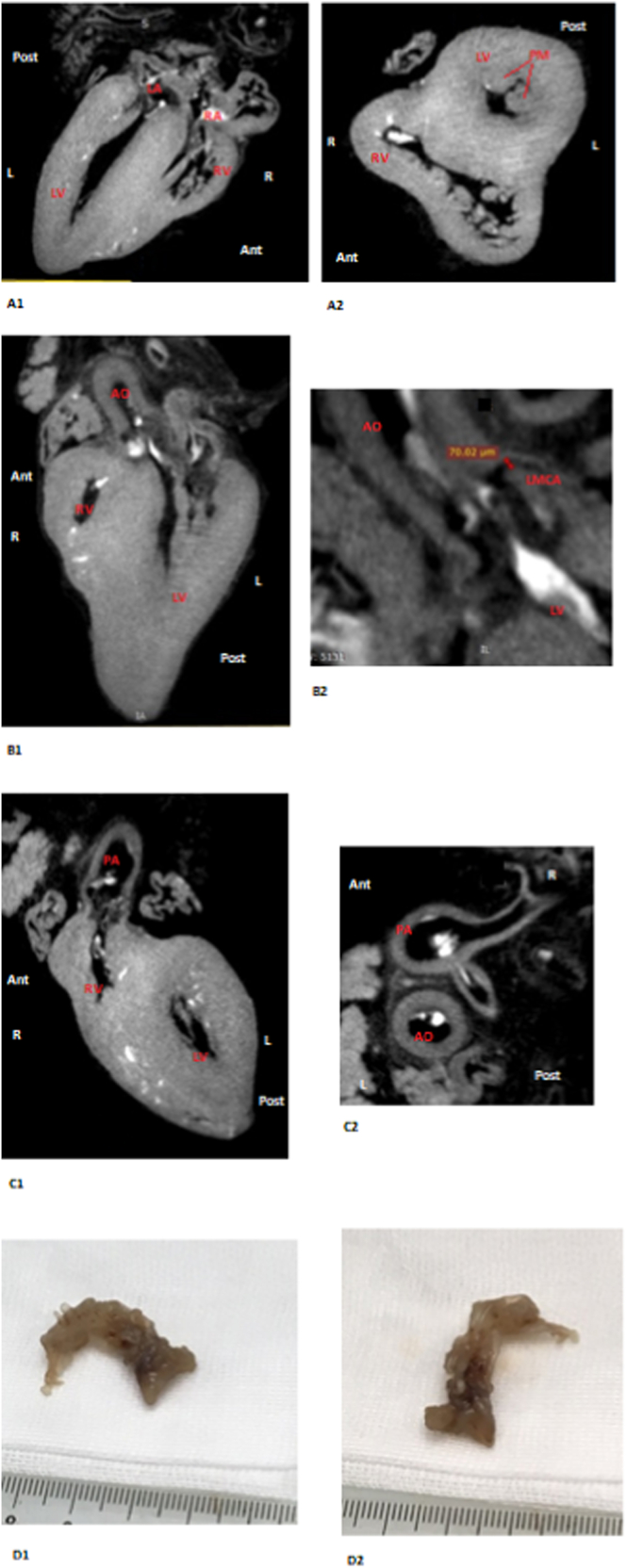
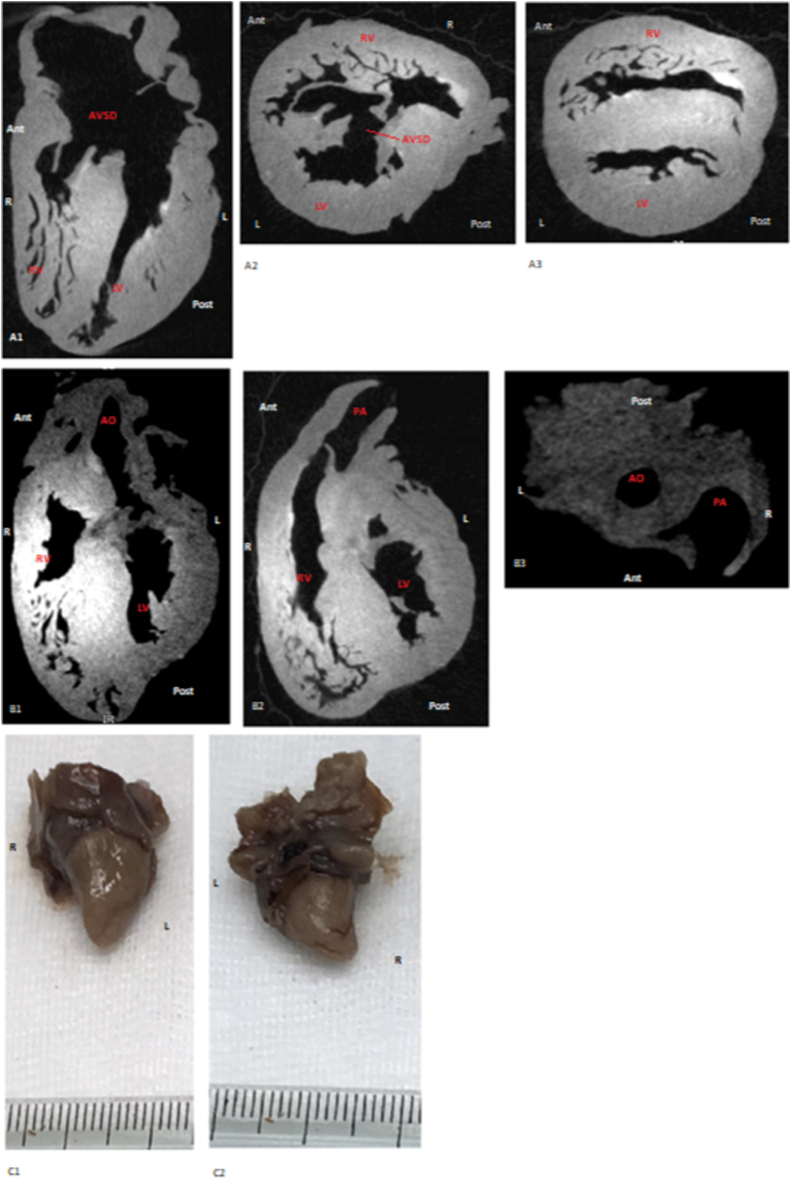
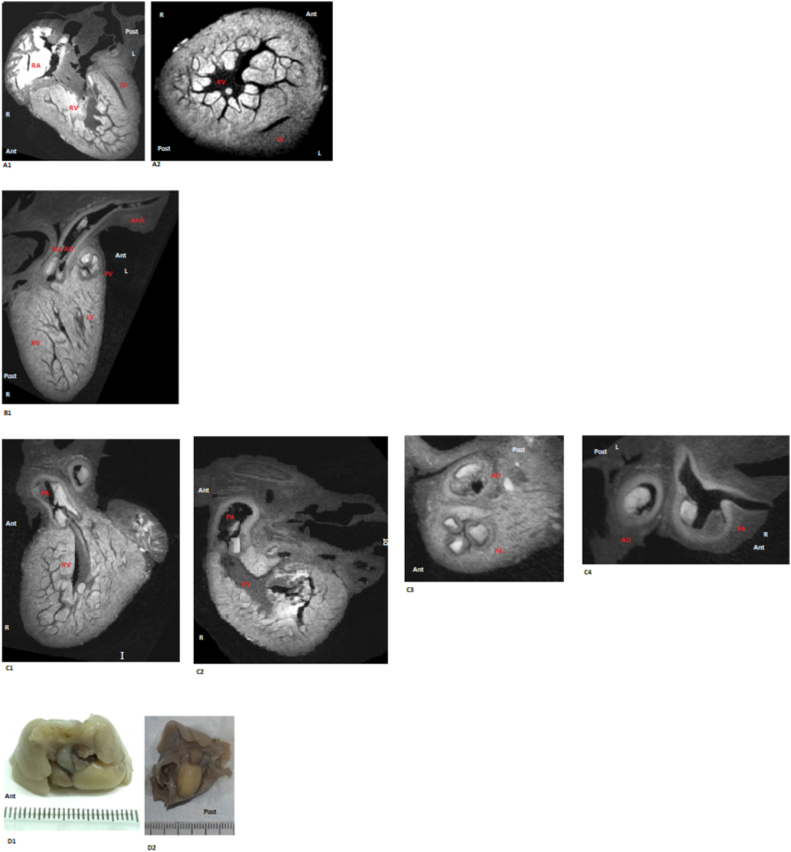
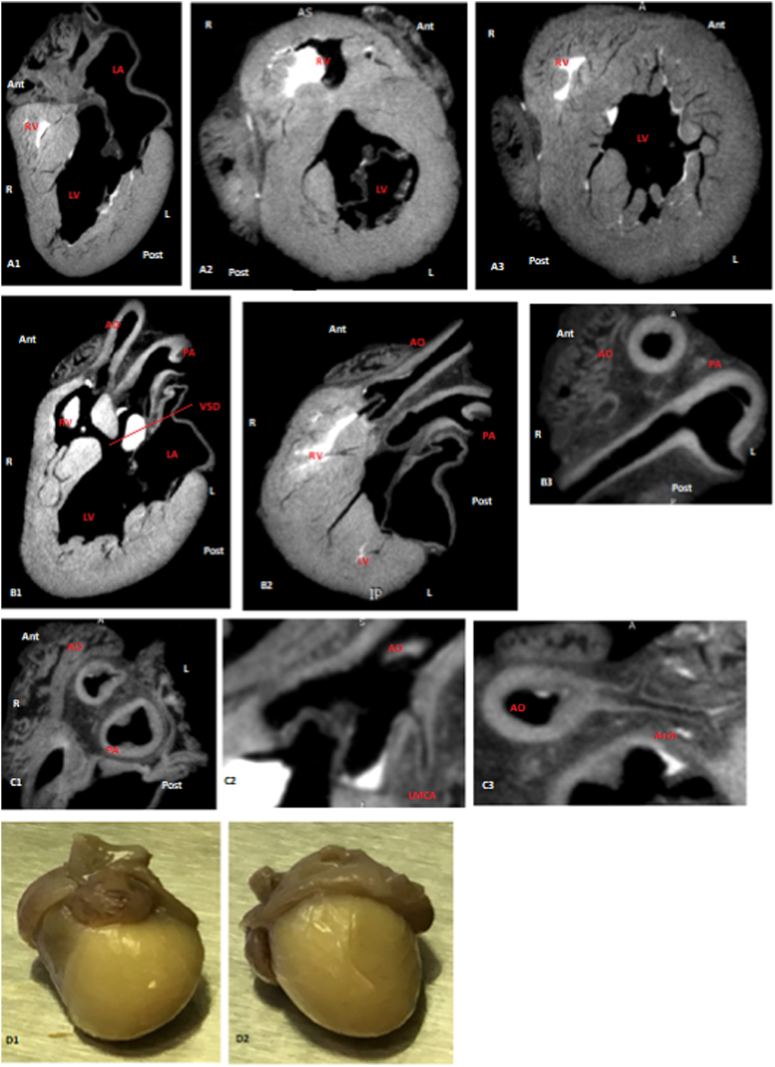
Background: Postmortem analysis of fetal heart is crucial but challenging. Alternative techniques to autopsy have been studied. We investigate micro-CT diagnostic accuracy in the analysis of fetal heart coming from early and late termination of pregnancy.
Methods: Micro-CT and autopsy analyzed human fetal heart using twenty-six indices of cardiac anatomy derived from segmental approach. Sub-analysis of smaller specimens was performed. Primary outcome is the agreement between techniques. Secondary outcomes are sensitivity, specificity, positive and negative predictive value. Indices are defined "visible" or "non-visible" (primary end point) and "normal", "abnormal" or "non-diagnostic" (secondary end point).
Results: Fifty-five cases were included. Agreement was 74.5% and 65.2% for primary end point and 93.3% and 91.8% for secondary end point in general population and in the group of smaller specimens, respectively. Sensitivity, specificity, positive and negative predictive value were 92.8%, 51.8%, 67.1%, 87.2% in the general population and 92.8%, 47.8%, 54.3%, 90.9% in the subgroup of smaller specimens for primary end point. They were 97.3%, 68.3%, 95.1%, 80.0% in the general population and 95.7%, 75.6%, 94.2%, 81.0% in the subgroup of smaller specimens for secondary end point. 86.1% and 91.5% of indices defined as "non-diagnostic" at autopsy would be visible by micro-CT in the two studied populations.
Conclusion: Micro-CT represents a valid alternative to autopsy for postmortem evaluation of human fetal heart. We proposed to use micro-CT for initial analysis of fetal heart and to perform autopsy only in unsolved cases or if histological analysis is needed.
Keywords: Congenital heart disease; Fetal heart; Micro-CT; Postmortem study; Virtual autopsy.
© 2021 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Clinical utility of postmortem microcomputed tomography of the fetal heart: diagnostic imaging vs macroscopic dissection.Ultrasound Obstet Gynecol. 2016 Jan;47(1):58-64. doi: 10.1002/uog.15764. Epub 2015 Dec 2. Ultrasound Obstet Gynecol. 2016. PMID: 26415141
-
Accuracy of Micro-Computed Tomography in Post-mortem Evaluation of Fetal Congenital Heart Disease. Comparison Between Post-mortem Micro-CT and Conventional Autopsy.Front Pediatr. 2019 Mar 22;7:92. doi: 10.3389/fped.2019.00092. eCollection 2019. Front Pediatr. 2019. PMID: 30968009 Free PMC article.
-
Postmortem Micro-CT of Human Fetal Heart-A Systematic Literature Review.J Clin Med. 2021 Oct 15;10(20):4726. doi: 10.3390/jcm10204726. J Clin Med. 2021. PMID: 34682849 Free PMC article. Review.
-
Diagnostic quality of 3Tesla postmortem magnetic resonance imaging in fetuses with and without congenital heart disease.Am J Obstet Gynecol. 2021 Aug;225(2):189.e1-189.e30. doi: 10.1016/j.ajog.2021.02.030. Epub 2021 Mar 1. Am J Obstet Gynecol. 2021. PMID: 33662361
-
Fetal postmortem imaging: an overview of current techniques and future perspectives.Am J Obstet Gynecol. 2020 Oct;223(4):493-515. doi: 10.1016/j.ajog.2020.04.034. Epub 2020 May 4. Am J Obstet Gynecol. 2020. PMID: 32376319 Review.
References
-
- Minnella G.P., Crupano F.M., Syngelaki A., Zidere V., Akolekar R., Nicolaides K.H. Diagnosis of major heart defects by routine first-trimester ultrasound examination: association with increased nuchal translucency, tricuspid regurgitation and abnormal flow in ductus venosus. Ultrasound Obstet Gynecol. 2020;55:637–644. doi: 10.1002/uog.21956. - DOI - PubMed
LinkOut - more resources
Full Text Sources
