

Common carotid artery characteristics in patients with repaired aortic coarctation compared to other cardiovascular risk factors
- PMID: 39712286
- PMCID: PMC11657401
- DOI: 10.1016/j.ijcchd.2022.100319
Common carotid artery characteristics in patients with repaired aortic coarctation compared to other cardiovascular risk factors
Abstract
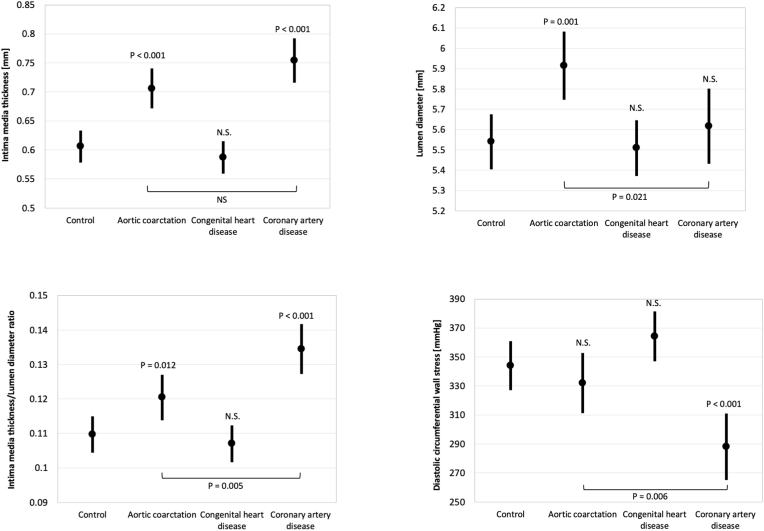
Aims: Increased common carotid artery (CCA) intima media thickness (cIMT) is a well-known risk factor for cardiovascular morbidity and mortality. cIMT thickening has been described in patients with repaired aortic coarctation (CoA), but data on mechanism and clinical relevance in this population are scarce. Our aim was to gain mechanistic insights into cIMT thickening of patients with repaired CoA by comparing their wall architecture to patients with coronary artery disease (CAD), other congenital heart diseases (oCHD), and healthy controls.
Methods and results: A total of 310 subjects were included (CoA (n = 58), oCHD (n = 96), CAD (n = 68) and healthy controls (n = 88)). CIMT and lumen diameter (LD) were determined using semiautomated analysis software. Linear regression analyses were performed correcting for relevant covariates. While patients with repaired CoA and CAD both had significantly increased cIMT and cIMT/LD ratios, LD was increased only in CoA patients. Furthermore, patients with repaired CoA had decreased CCA stiffness. CCA characteristics in the oCHD group were not significantly different from controls.
Conclusion: The mechanism of cIMT thickening in patients with repaired CoA may differ from CAD. While there is concentric remodeling in the latter, we see predominant eccentric remodeling in the CoA group, which could be due to increased flow as a result of compliance mismatch at the CoA repair site. We therefore suggest that the prognostic value of cIMT in post-CoA patients should be validated separately prior to using it to guide clinical management in this group.
Keywords: Aortic coarctation; Arterial stiffness; Common carotid artery; Congenital heart disease; Dimension; Intima media thickness.
© 2022 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


Similar articles
-
Increased blood pressure is associated with increased carotid artery intima-media thickness in children with repaired coarctation of the aorta.J Hypertens. 2019 Aug;37(8):1689-1698. doi: 10.1097/HJH.0000000000002077. J Hypertens. 2019. PMID: 30950974
-
Increased carotid intima-media thickness predicts cardiovascular events in aortic coarctation.Int J Cardiol. 2014 Oct 20;176(3):776-81. doi: 10.1016/j.ijcard.2014.07.090. Epub 2014 Aug 17. Int J Cardiol. 2014. PMID: 25205481
-
Carotid intima-media thickness is increased in patients with treated mucopolysaccharidosis types I and II, and correlates with arterial stiffness.Mol Genet Metab. 2014 Feb;111(2):128-32. doi: 10.1016/j.ymgme.2013.11.001. Epub 2013 Nov 12. Mol Genet Metab. 2014. PMID: 24268528 Free PMC article.
-
Varying Definitions of Carotid Intima-Media Thickness and Future Cardiovascular Disease: A Systematic Review and Meta-Analysis.J Am Heart Assoc. 2023 Dec 5;12(23):e031217. doi: 10.1161/JAHA.123.031217. Epub 2023 Nov 28. J Am Heart Assoc. 2023. PMID: 38014663 Free PMC article.
-
Carotid intima-media thickness testing as an asymptomatic cardiovascular disease identifier and method for making therapeutic decisions.Postgrad Med. 2013 Mar;125(2):108-23. doi: 10.3810/pgm.2013.03.2645. Postgrad Med. 2013. PMID: 23816777 Review.
Cited by
-
Coarctation of the aorta and accelerated atherosclerosis: A contemporary review on the burden of atherosclerotic cardiovascular disease.Int J Cardiol Congenit Heart Dis. 2024 Dec 25;19:100561. doi: 10.1016/j.ijcchd.2024.100561. eCollection 2025 Mar. Int J Cardiol Congenit Heart Dis. 2024. PMID: 39926128 Free PMC article.
-
Impact of smoking on cardiovascular health: Mechanisms, epidemiology and specific concerns regarding congenital heart disease.Int J Cardiol Congenit Heart Dis. 2025 Apr 2;20:100581. doi: 10.1016/j.ijcchd.2025.100581. eCollection 2025 Jun. Int J Cardiol Congenit Heart Dis. 2025. PMID: 40242035 Free PMC article. Review.
-
Relationship between elevated homocysteine levels and the degree of white matter lesions in stroke patients.Medicine (Baltimore). 2025 Apr 4;104(14):e41984. doi: 10.1097/MD.0000000000041984. Medicine (Baltimore). 2025. PMID: 40193635 Free PMC article.
References
-
- Warnes C.A., Williams R.G., Bashore T.M., Child J.S., Connolly H.M., Dearani J.A., et al. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: executive summary: a report of the American college of cardiology/American heart association task force on practice guidelines (writing committee to develop guidelines for the management of adults with congenital heart disease) Circulation. 2008;118(23):2395–2451. - PubMed
-
- Baumgartner H., Bonhoeffer P., De Groot N.M., de Haan F., Deanfield J.E., Galie N., et al. ESC Guidelines for the management of grown-up congenital heart disease (new version 2010) Eur Heart J. 2010;31(23):2915–2957. - PubMed
-
- Roifman I., Therrien J., Ionescu-Ittu R., Pilote L., Guo L., Kotowycz M.A., et al. Coarctation of the aorta and coronary artery disease: fact or fiction? Circulation. 2012;126(1):16–21. - PubMed
-
- Reiner B., Oberhoffer R., Hacker A.L., Ewert P., Muller J. Carotid intima-media thickness in children and adolescents with congenital heart disease. Can J Cardiol. 2018;34(12):1618–1623. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
