

A Case of Antenatal Diagnosis of Absent Pulmonary Valve Syndrome with Intact Ventricular Septum, Large Patent Ductus Arteriosus, and Ascending Aorta Dilatation
- PMID: 39712357
- PMCID: PMC11659710
- DOI: 10.18502/jthc.v19i1.15614
A Case of Antenatal Diagnosis of Absent Pulmonary Valve Syndrome with Intact Ventricular Septum, Large Patent Ductus Arteriosus, and Ascending Aorta Dilatation
Abstract
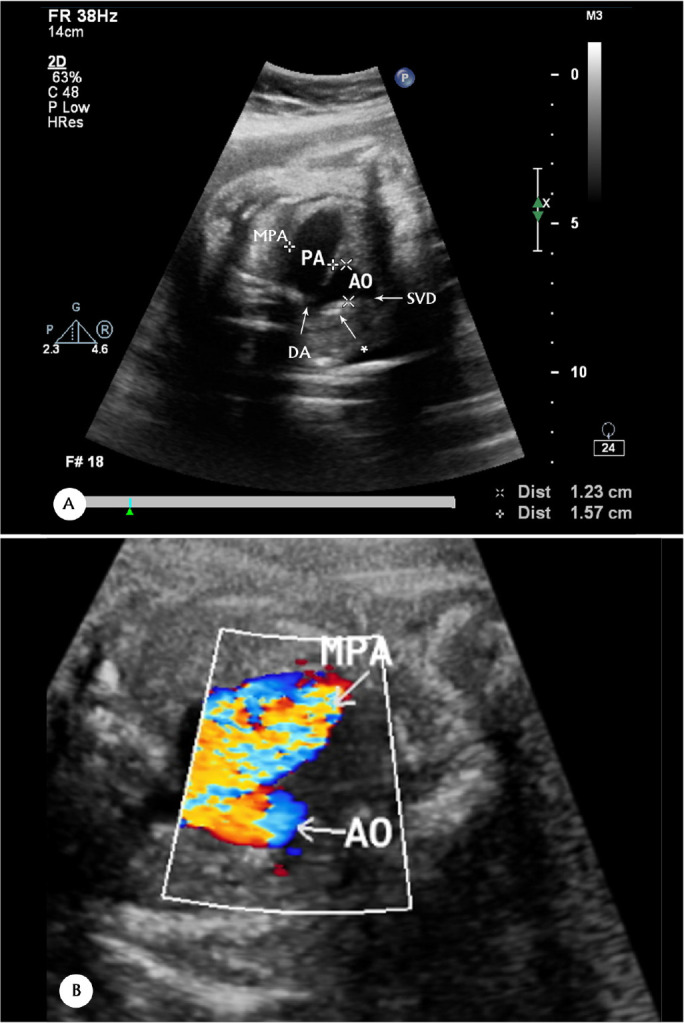
Absent pulmonary valve syndrome (APVS) is a rare congenital anomaly characterized by rudimentary PV tissue with variable degrees of PV stenosis and regurgitant pulmonary blood flow. In most cases, it is associated with tetralogy of Fallot. In a minority of APVS cases, with an unknown frequency, intact ventricular septum (IVS), patent ductus arteriosus, and possible tricuspid atresia are present. This condition is known as non-Fallot type APVS. We describe a case of an antenatal diagnosis of APVS with IVS, a large patent ductus arteriosus, and ascending aorta dilatation. The mother was referred to our center at 32 weeks of gestation due to cardiomegaly on sonography. Fetal echocardiography revealed cardiomegaly, right atrial and ventricular enlargement, aneurysmal dilatation of the main pulmonary artery, and mild dilatation of the pulmonary artery branches. Also observed were IVS, rudimentary PV tissue with severe to-and-fro turbulence across the PV, a widely open ductus arteriosus, ascending aorta dilatation, and levorotation of the heart. After childbirth, our diagnosis was confirmed by echocardiography and surgery. The baby experienced severe respiratory distress. At 15 days of life, surgical intervention in the form of pulmonary artery arterioplasty was performed, resulting in good outcomes. The patient underwent follow-up for 6 months and showed reasonable health.
Keywords: Antenatal diagnosis; Pulmonary valve incompetence; Pulmonary valve/abnormalities*.
Copyright© 2024 Tehran University of Medical Sciences. Published by Tehran University of Medical Sciences.
Figures








Similar articles
-
Absent Pulmonary Valve Syndrome in a Fetus: A Case Report and Literature Review.Fetal Pediatr Pathol. 2019 Feb;38(1):57-62. doi: 10.1080/15513815.2018.1529066. Epub 2019 Jan 20. Fetal Pediatr Pathol. 2019. PMID: 30661433 Review.
-
Prenatal diagnosis of absent pulmonary valve syndrome: report of 2 cases, most common and most rare presentations.J Ultrasound Med. 2010 May;29(5):823-9. doi: 10.7863/jum.2010.29.5.823. J Ultrasound Med. 2010. PMID: 20427795
-
'Absent' pulmonary valve with intact ventricular septum mimicking tricuspid valve atresia: Prenatal diagnosis and postnatal course.J Obstet Gynaecol Res. 2019 Mar;45(3):714-718. doi: 10.1111/jog.13878. Epub 2019 Jan 17. J Obstet Gynaecol Res. 2019. PMID: 30656796
-
Prenatal Diagnosis, Associations and Outcome for Fetuses with Congenital Absence of the Pulmonary Valve Syndrome.Anatol J Cardiol. 2022 Sep;26(9):702-709. doi: 10.5152/AnatolJCardiol.2022.1461. Anatol J Cardiol. 2022. PMID: 35943311 Free PMC article.
-
Absent pulmonary valve syndrome with tetralogy of fallot and patent ductus arteriosus at 14 weeks of gestation and follow-up 2 weeks later: Case report and review of literature.Echocardiography. 2021 Mar;38(3):484-487. doi: 10.1111/echo.14936. Epub 2021 Feb 5. Echocardiography. 2021. PMID: 33544401 Review.
References
-
- Grotenhuis HB, Nijveld A, Backx A. Absent pulmonary valve syndrome with intact ventricular septum and patent ductus arteriosus: report of two cases and a short review of the literature. Ann Thorac Surg 2003;75:280–282. - PubMed
-
- Podzimkova J, Hickey MS, Slavik Z, Leanage R, Chan KC. Absent pulmonary valve syndrome with intact ventricular septum: role of ductus arteriosus revisited. Int J Cardiol 1997;61:109–112. - PubMed
-
- Rabinovitch M, Grady S, David I, Van Praagh R, Sauer U, Buhlmeyer K, Castaneda AR, Reid L. Compression of intrapulmonary bronchi by abnormally branching pulmonary arteries associated with absent pulmonary valves. Am J Cardiol 1982;50:804–813. - PubMed
-
- Gottschalk I, Jehle C, Herberg U, Breuer J, Brockmeier K, Bennink G, Hellmund A, Strizek B, Gembruch U, Geipel A, Berg C. Prenatal diagnosis of absent pulmonary valve syndrome from first trimester onwards: novel insights into pathophysiology, associated conditions and outcome. Ultrasound Obstet Gynecol 2017;49:637–642. - PubMed
-
- Karimi A, Peiravian F, Amirghofran AA, Kariminejad A. Absent pulmonary valve, intact interventricular septum, rudimentary aortic non-coronary cusp and ascending aortic aneurysm in a single patient. Interact Cardiovasc Thorac Surg 2010;10:636–638. - PubMed
Publication types
LinkOut - more resources
Full Text Sources