

Metastatic brain tumors: from development to cutting-edge treatment
- PMID: 39712454
- PMCID: PMC11661909
- DOI: 10.1002/mco2.70020
Metastatic brain tumors: from development to cutting-edge treatment
Abstract
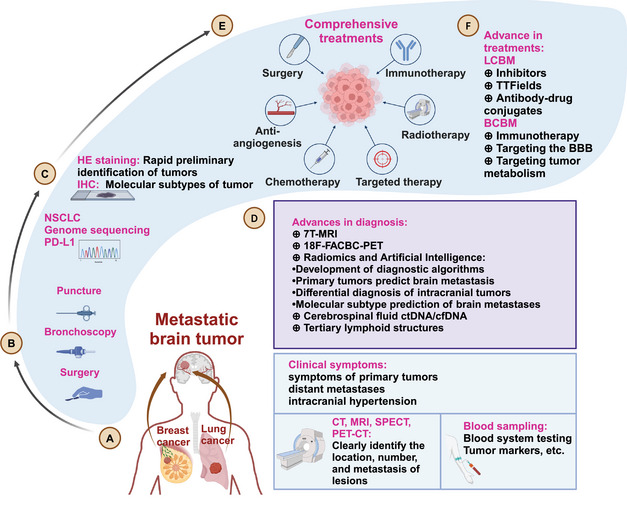
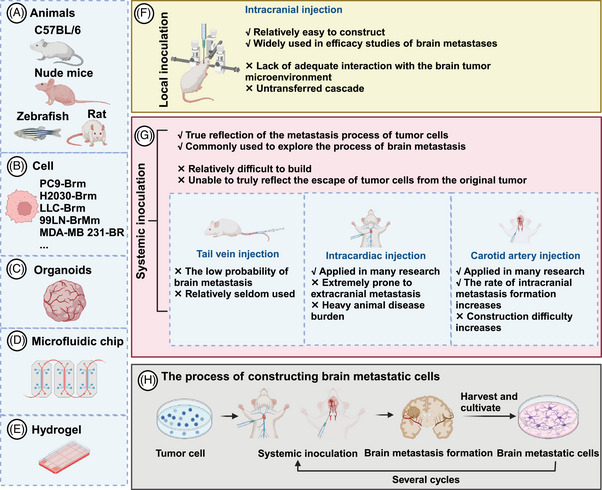
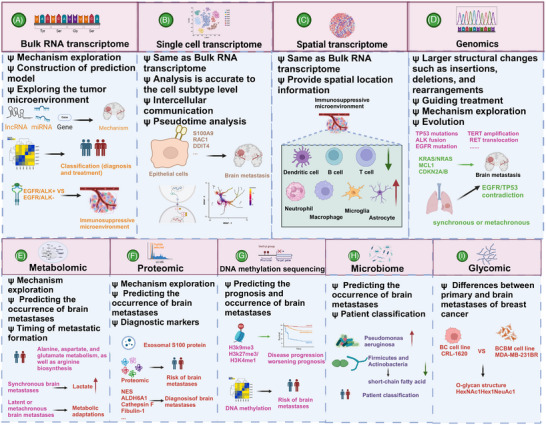
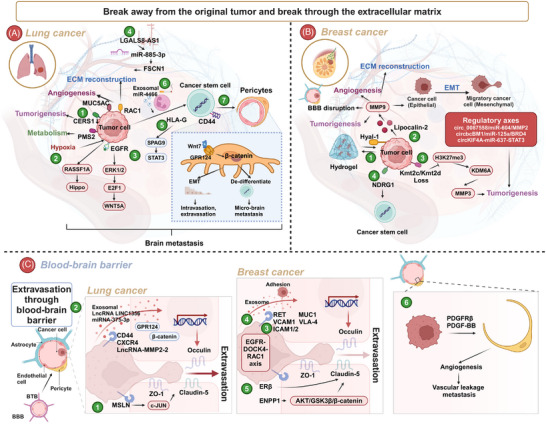
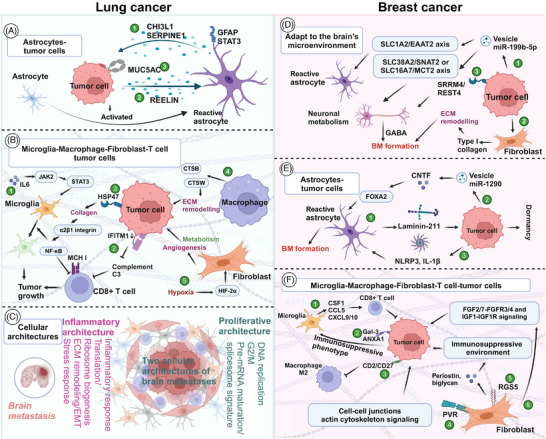
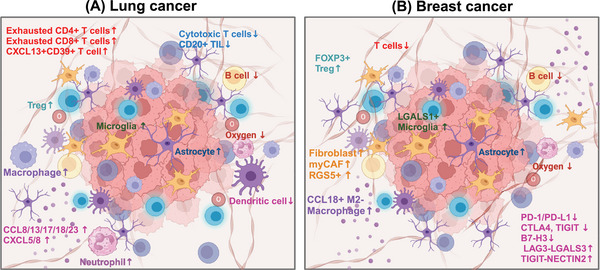
Metastatic brain tumors, also called brain metastasis (BM), represent a challenging complication of advanced tumors. Tumors that commonly metastasize to the brain include lung cancer and breast cancer. In recent years, the prognosis for BM patients has improved, and significant advancements have been made in both clinical and preclinical research. This review focuses on BM originating from lung cancer and breast cancer. We briefly overview the history and epidemiology of BM, as well as the current diagnostic and treatment paradigms. Additionally, we summarize multiomics evidence on the mechanisms of tumor occurrence and development in the era of artificial intelligence and discuss the role of the tumor microenvironment. Preclinically, we introduce the establishment of BM models, detailed molecular mechanisms, and cutting-edge treatment methods. BM is primarily treated with a comprehensive approach, including local treatments such as surgery and radiotherapy. For lung cancer, targeted therapy and immunotherapy have shown efficacy, while in breast cancer, monoclonal antibodies, tyrosine kinase inhibitors, and antibody-drug conjugates are effective in BM. Multiomics approaches assist in clinical diagnosis and treatment, revealing the complex mechanisms of BM. Moreover, preclinical agents often need to cross the blood-brain barrier to achieve high intracranial concentrations, including small-molecule inhibitors, nanoparticles, and peptide drugs. Addressing BM is imperative.
Keywords: diagnosis and treatment; metastatic brain tumors; molecular mechanisms; multiomics; tumor microenvironment.
© 2024 The Author(s). MedComm published by Sichuan International Medical Exchange & Promotion Association (SCIMEA) and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
The authors declare that there is no conflict of interest in any aspect.
Figures
Similar articles
-
Where Are We Now and Where Might We Be Headed in Understanding and Managing Brain Metastases in Colorectal Cancer Patients?Curr Treat Options Oncol. 2022 Jul;23(7):980-1000. doi: 10.1007/s11864-022-00982-0. Epub 2022 Apr 28. Curr Treat Options Oncol. 2022. PMID: 35482170 Free PMC article. Review.
-
Tumor Immune Microenvironment and Immunotherapy in Brain Metastasis From Non-Small Cell Lung Cancer.Front Immunol. 2022 Feb 17;13:829451. doi: 10.3389/fimmu.2022.829451. eCollection 2022. Front Immunol. 2022. PMID: 35251014 Free PMC article. Review.
-
Unlocking the Role of Metabolic Pathways in Brain Metastatic Disease.Cells. 2025 May 13;14(10):707. doi: 10.3390/cells14100707. Cells. 2025. PMID: 40422210 Free PMC article. Review.
-
Brain metastases in metastatic cancer: a review of recent advances in systemic therapies.Expert Rev Anticancer Ther. 2021 Mar;21(3):325-339. doi: 10.1080/14737140.2021.1851200. Epub 2020 Nov 30. Expert Rev Anticancer Ther. 2021. PMID: 33196341 Review.
-
Immunotherapeutic and Targeted Strategies for Managing Brain Metastases from Common Cancer Origins: A State-of-the-Art Review.Curr Oncol Rep. 2024 Dec;26(12):1612-1638. doi: 10.1007/s11912-024-01593-8. Epub 2024 Nov 8. Curr Oncol Rep. 2024. PMID: 39514054 Review.
Cited by
-
Current Bioinformatics Tools in Precision Oncology.MedComm (2020). 2025 Jul 9;6(7):e70243. doi: 10.1002/mco2.70243. eCollection 2025 Jul. MedComm (2020). 2025. PMID: 40636286 Free PMC article. Review.
-
Medulloblastoma: biology and immunotherapy.Front Immunol. 2025 Jul 3;16:1602930. doi: 10.3389/fimmu.2025.1602930. eCollection 2025. Front Immunol. 2025. PMID: 40677711 Free PMC article. Review.
References
-
- Boire A, Brastianos PK, Garzia L, Valiente M. Brain metastasis. Nat Rev Cancer. 2020;20(1):4‐11. - PubMed
-
- Relli V, Trerotola M, Guerra E, Alberti S. Abandoning the notion of non‐small cell lung cancer. Trends Mol Med. 2019;25(7):585‐594. - PubMed
-
- Gillespie CS, Mustafa MA, Richardson GE, et al. Genomic alterations and the incidence of brain metastases in advanced and metastatic NSCLC: a systematic review and meta‐analysis. J Thorac Oncol. 2023;18(12):1703‐1713. - PubMed
Publication types
LinkOut - more resources
Full Text Sources