

Development of Modic Changes After Percutaneous Endoscopic Transforaminal Lumbar Discectomy: From Risk Analysis to Prediction Modeling
- PMID: 39712462
- PMCID: PMC11662668
- DOI: 10.2147/JPR.S475650
Development of Modic Changes After Percutaneous Endoscopic Transforaminal Lumbar Discectomy: From Risk Analysis to Prediction Modeling
Abstract
Objective: This study examines the occurrence of Modic changes (MC) within the first year following percutaneous endoscopic transforaminal lumbar discectomy (PETD) and investigates associated risk factors.
Methods: This study adopted a retrospective cohort design. Between January 2019 and June 2023, 538 patients diagnosed with single-level lumbar disc herniation and treated with PETD were included. The patients were divided into a training set and a validation set based on their surgery dates. Preoperative radiographic parameters and perioperative indicators were evaluated. Univariate analysis examined risk factors for postoperative MC. Gender-specific subgroups were analyzed. Binary logistic regression developed a predictive model for postoperative MC, assessed using ROC, calibration, and decision curves.
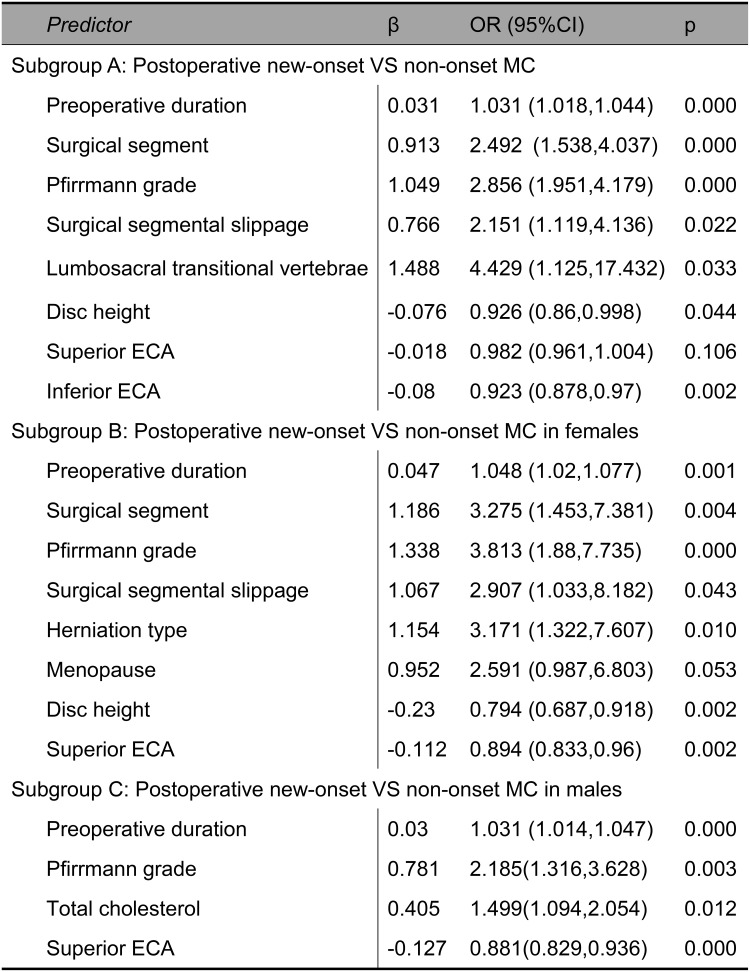
Results: The incidence of MC at one year after PETD was 24.8%. Logistic regression identified 8 significant risk factors for MC after PELD: longer symptom duration, proximity of herniated segment to sacrum, severe disc degeneration, reduced disc height, greater vertebral endplate concavity angle, segmental instability, and lumbar-sacral fusion. Menopause and herniation type were identified as female-specific risk factors. In males, total cholesterol levels were additionally found to be a risk factor for postoperative MC. The male and female subgroup models exhibited satisfactory performance across ROC analysis, calibration plots, and decision curve analysis. Specifically, for male patients, the area under the curve (AUC) was 0.831 for the training set and 0.820 for the validation set; for female patients, the AUC was 0.911 for the training set and 0.868 for the validation set. A nomogram was developed to visualize the model.
Conclusion: This study explored the relevant risk factors of MC after PETD and visualized the prediction model by nomogram, which is beneficial to optimize the surgical scheme of PETD to improve the clinical efficacy.
Keywords: Modic changes; lumbar disc disease; percutaneous endoscopic transforaminal discectomy; risk analysis.
© 2024 Li et al.
Conflict of interest statement
The authors have nothing to disclose.
Figures


References
LinkOut - more resources
Full Text Sources
