

Concordance of Extent of Resection Between Intraoperative Ultrasound and Postoperative MRI in Brain and Spine Tumor Resection
- PMID: 39712672
- PMCID: PMC11661696
- DOI: 10.7759/cureus.74101
Concordance of Extent of Resection Between Intraoperative Ultrasound and Postoperative MRI in Brain and Spine Tumor Resection
Abstract
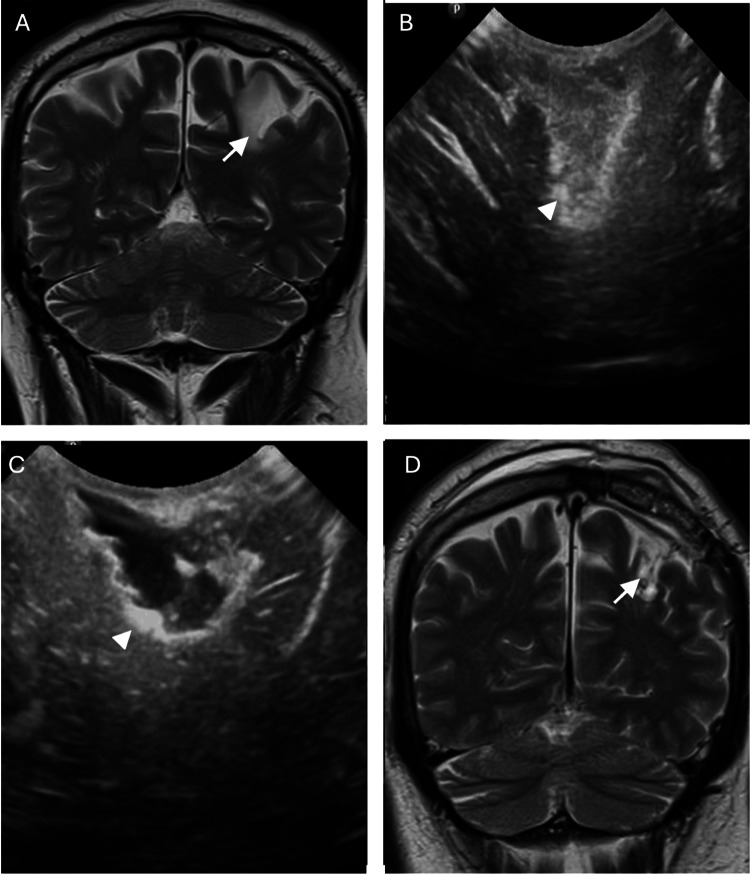
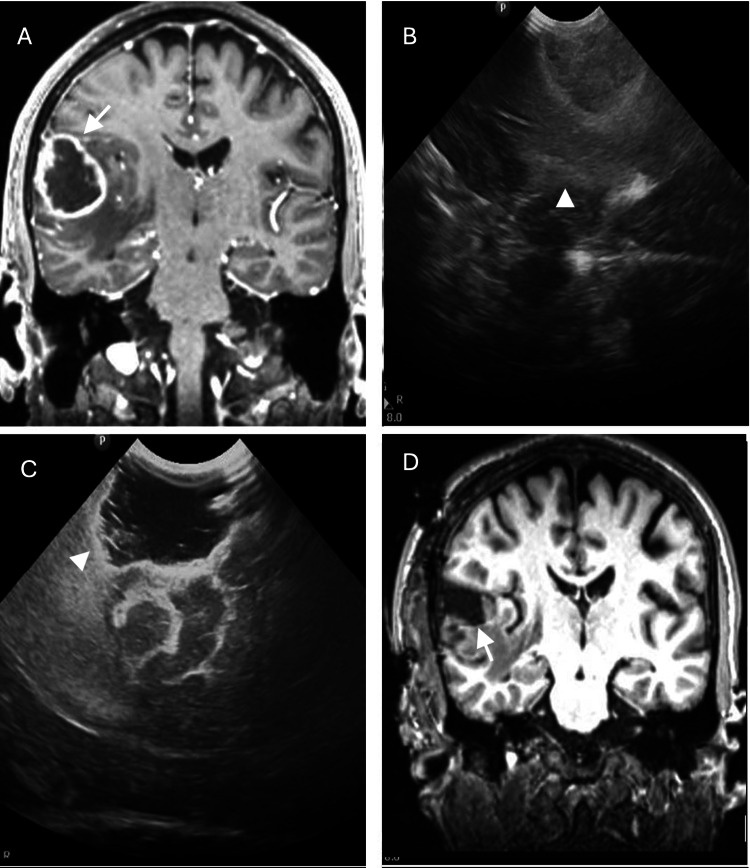
Objective Evaluate the utility of intraoperative ultrasound (IOUS) in brain and spinal tumor resections and the concordance of the extent of resection between IOUS and postoperative magnetic resonance imaging (MRI). Methods A retrospective analysis of prospectively collected data was performed. Thirty-nine lesions (36 patients) in the brain and spine were operated on for resection using IOUS between May 2020 and December 2022. All patients who underwent brain or spinal tumor resection were included, and who underwent IOUS during tumor resection and postoperative MRI was done within 48 hours of surgery. The Cohen's kappa coefficient was performed to the concordance of resection by IOUS and postoperative MRI. Results Forty-one patients underwent surgery, of which 36 met the inclusion criteria and five were excluded due to incomplete clinical records. Of the 36 patients included, two presented lesions in different locations, one with frontal and parietal metastases and the other with extradural and intradural spinal lesions, and one patient had a recurrence of glioblastoma, for which 39 procedures were included. Of the 36 patients, 36% were women, and the average age was 51.4 years with an age range of one year and two months to 94 years. The concordance of the degree of resection by ultrasound and the degree of resection by postoperative magnetic resonance is high. Conclusions The higher degree of concordance between IOUS and postoperative MRI would suggest that IOUS is a reliable tool for assessing the extent of tumor resection during surgery and provides real-time information to make decisions to adjust surgery plans based on the benefit/risk ratio.
Keywords: brain tumor; intraoperative ultrasound; magnetic resonance image; neurosurgery; oncology; spine tumor; tumor resection.
Copyright © 2024, Caro-Osorio et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Institutional Review Board of Tecnologico de Monterrey, Monterrey, Mexico issued approval NA. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Correlation between intraoperative ultrasound and postoperative MRI in pediatric tumor surgery.J Neurosurg Pediatr. 2016 Nov;18(5):578-584. doi: 10.3171/2016.5.PEDS15739. Epub 2016 Jul 29. J Neurosurg Pediatr. 2016. PMID: 27472668
-
Efficacy of intraoperative ultrasonography in neurosurgical tumor resection.J Neurosurg Pediatr. 2018 May;21(5):504-510. doi: 10.3171/2017.11.PEDS17473. Epub 2018 Feb 16. J Neurosurg Pediatr. 2018. PMID: 29451454
-
Intraoperative Ultrasound-Assisted Extent of Resection Assessment in Pediatric Neurosurgical Oncology.Front Oncol. 2021 Apr 21;11:660805. doi: 10.3389/fonc.2021.660805. eCollection 2021. Front Oncol. 2021. PMID: 33968768 Free PMC article.
-
Evaluating intraoperative ultrasound (IOUS) in focal cortical dysplasia (FCD) resection surgery: A systematic review.Surg Neurol Int. 2024 May 17;15:165. doi: 10.25259/SNI_109_2024. eCollection 2024. Surg Neurol Int. 2024. PMID: 38840597 Free PMC article. Review.
-
New Hope in Brain Glioma Surgery: The Role of Intraoperative Ultrasound. A Review.Brain Sci. 2018 Nov 19;8(11):202. doi: 10.3390/brainsci8110202. Brain Sci. 2018. PMID: 30463249 Free PMC article. Review.
References
-
- The human brain in depth: how we see in 3D. Welchman AE. Annu Rev Vis Sci. 2016;2:345–376. - PubMed
-
- Intraoperative MRI in pediatric brain tumors. Choudhri AF, Siddiqui A, Klimo P Jr, Boop FA. Pediatr Radiol. 2015;45 Suppl 3:0–405. - PubMed
-
- Intraoperative MRI and maximizing extent of resection. Rao G. Neurosurg Clin N Am. 2017;28:477–485. - PubMed
-
- Intraoperative high-field resonance: how to optimize its use in our healthcare system. Limpo H, Díez R, Albisua J, Tejada S. Neurocirugia (Astur: Engl Ed) 2022;33:261–268. - PubMed
-
- Intraoperative MRI guidance and extent of resection in glioma surgery: a randomised, controlled trial. Senft C, Bink A, Franz K, Vatter H, Gasser T, Seifert V. Lancet Oncol Oct. 2011;12:997–1003. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous