

Branch Retinal Artery Occlusion as a Presentation of Seronegative Antiphospholipid Syndrome in Pregnancy
- PMID: 39712706
- PMCID: PMC11663242
- DOI: 10.7759/cureus.74198
Branch Retinal Artery Occlusion as a Presentation of Seronegative Antiphospholipid Syndrome in Pregnancy
Abstract
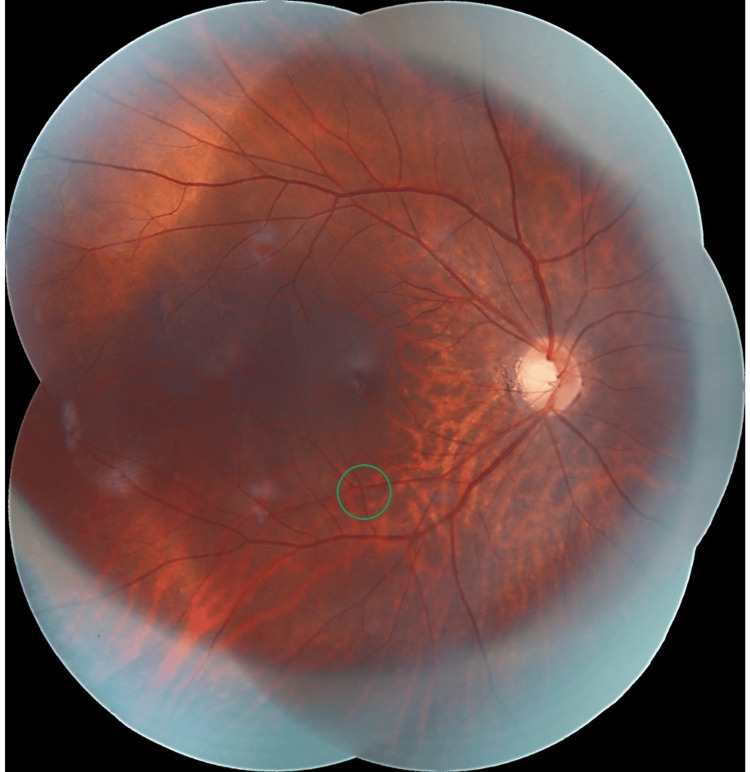
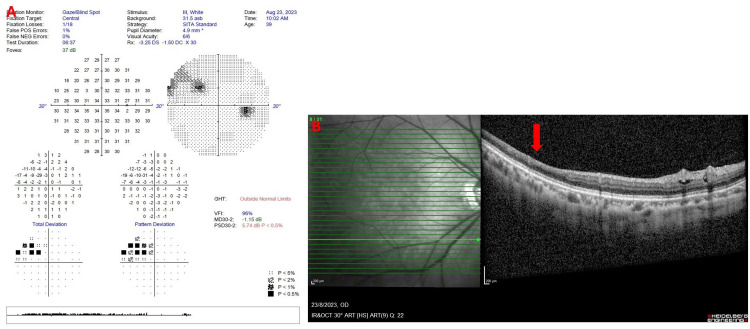
A 40-year-old gravida 7 para 4+2 lady who was 14 weeks pregnant presented with a three-day history of sudden-onset flashes of light associated with a superonasal visual field defect on her right eye. She had two prior miscarriages that occurred in the second and third trimesters. Previous serological tests for antiphospholipid syndrome (APS) were normal. No other comorbidities were reported. On examination, visual acuity for both eyes was 6/6 with normal intra-ocular pressure. There was an embolus lodged at the inferotemporal peripheral retinal artery of the right eye with adjacent pale and oedematous distal retina. This corresponded with a superonasal scotoma on the Humphrey 30-2 visual field test. Other examinations were unremarkable. The patient was referred to obstetrics, rheumatology, and neuro-medical teams for co-management. Full blood count, coagulation profile, auto-immune panel, and antiphospholipid serological screening test were normal. No abnormalities were seen on her electrocardiogram and echocardiogram. A magnetic resonance angiogram of the brain revealed significant bilateral internal carotid stenosis at C2 and C6 levels. However carotid artery assessment showed normal flow below the jawline. The patient was diagnosed with seronegative APS with right-eye inferotemporal branch retinal artery occlusion (BRAO). A multidisciplinary team monitored her pregnancy, and she was started on subcutaneous enoxaparin 40 mg twice a day and oral aspirin/glycine 100 mg/45 mg once daily. At 20 weeks of pregnancy, the Hollenhorst plaque disappeared, and the visual field defect started to improve. She went on to deliver a healthy child at 36+6 weeks. Post-partum, she has continued on oral aspirin 100 mg once daily. A carotid angiogram performed post-delivery showed no evidence of internal carotid artery stenosis or thrombosis. This case highlights the importance of recognizing BRAO as it can be the presentation of a previously unrecognized seronegative antiphospholipid syndrome. Early recognition of the correct diagnosis is vital to allow effective multidisciplinary management, especially when dealing with a patient in pregnancy.
Keywords: antiphospholipid syndrome; branch retinal artery occlusion; ophthalmology; pregnancy; seronegative.
Copyright © 2024, Chewa Raja et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures


References
-
- Pregnancy and retinal and retinal vascular complications. Bhattacharya A, Arepalli SR. Ann Eye Sci. 2023;8:19.
-
- Central retinal artery occlusion, reduced to inferotemporal branch retinal artery occlusion in an otherwise healthy full term pregnant patient: a case report. Kanellopoulos AJ. https://www.scholarena.com/article/Central-Retinal-Artery-Occlusions.pdf J Clin Trials Rep. 2023;1:1–8.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous