

Sinonasal Carcinoma With Aggressive Right Intraorbital Extension and Left Eye Invasion in a Young Female Patient
- PMID: 39712724
- PMCID: PMC11659919
- DOI: 10.7759/cureus.74066
Sinonasal Carcinoma With Aggressive Right Intraorbital Extension and Left Eye Invasion in a Young Female Patient
Abstract
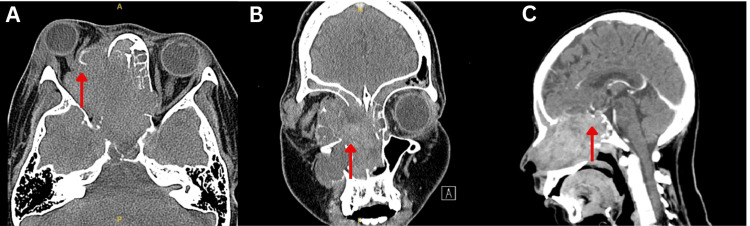
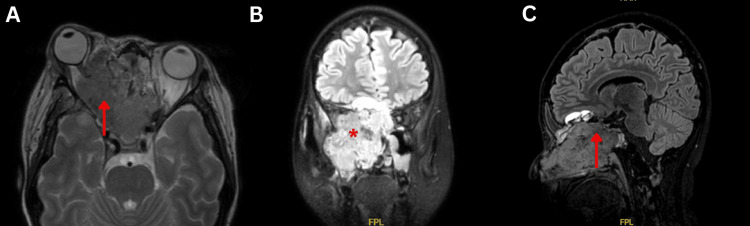
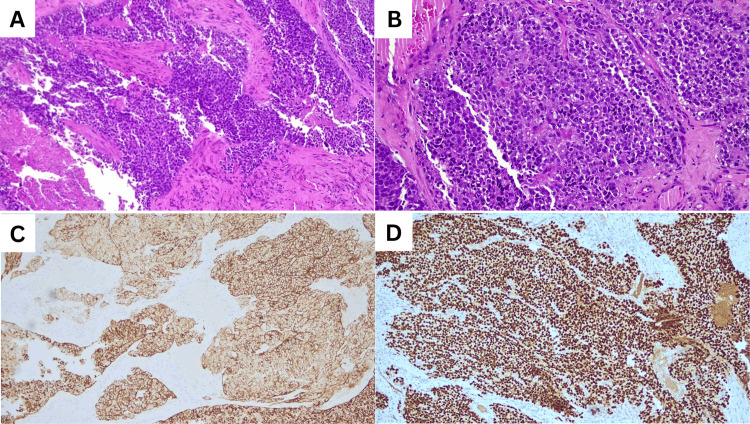
Sinonasal cancers are rare and aggressive head and neck malignancies. Sinonasal squamous cell carcinoma (SNSCC) typically affects males and individuals over the age of 55. Here, we present an unusual case of a young female diagnosed with SNSCC. She presented with painful right eye proptosis, rapid progressive vision loss in both eyes, and a history of intermittent epistaxis. MRI revealed an aggressive sinonasal mass with intra-orbital and intracranial extension, and a biopsy confirmed sinonasal non-keratinizing squamous cell carcinoma. Despite initial systemic chemotherapy, the patient discontinued treatment and, unfortunately, succumbed to the disease. This case highlights the aggressive nature and management challenges of advanced SNSCC, emphasizing the critical importance of early diagnosis and timely intervention to improve outcomes.
Keywords: bilateral intraorbital extension; intracranial extension; proptosis; sinonasal carcinoma; snscc.
Copyright © 2024, Mohd Ghazali et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
A Case Report of Sinonasal Primary Squamous Cell Carcinoma.Indian J Otolaryngol Head Neck Surg. 2024 Jun;76(3):2837-2839. doi: 10.1007/s12070-023-04459-w. Epub 2024 Feb 7. Indian J Otolaryngol Head Neck Surg. 2024. PMID: 38883524 Free PMC article.
-
Sinonasal Lymphoepithelial Carcinoma With Aggressive Orbital Invasion.Cureus. 2022 Nov 4;14(11):e31103. doi: 10.7759/cureus.31103. eCollection 2022 Nov. Cureus. 2022. PMID: 36475167 Free PMC article.
-
Chronic invasive fungal rhinosinusitis vs sinonasal squamous cell carcinoma: the differentiating value of MRI.Eur Radiol. 2020 Aug;30(8):4466-4474. doi: 10.1007/s00330-020-06838-1. Epub 2020 Apr 11. Eur Radiol. 2020. PMID: 32279114
-
Induction Chemotherapy for Locoregionally Advanced Sinonasal Squamous Cell Carcinoma and Sinonasal Undifferentiated Carcinoma: A Comprehensive Review.Cancers (Basel). 2023 Jul 26;15(15):3798. doi: 10.3390/cancers15153798. Cancers (Basel). 2023. PMID: 37568614 Free PMC article. Review.
-
Metastatic SMARCB1 (INI-1)-Deficient Sinonasal Carcinoma Diagnosed by Endobronchial Ultrasound-Guided Fine-Needle Aspiration (EBUS-FNA): A Potential Diagnostic Pitfall and Review of the Literature.Acta Cytol. 2019;63(5):431-437. doi: 10.1159/000500351. Epub 2019 May 27. Acta Cytol. 2019. PMID: 31132763 Review.
References
-
- Epidemiology of sinonasal squamous cell carcinoma: a comprehensive analysis of 4994 patients. Sanghvi S, Khan MN, Patel NR, Yeldandi S, Baredes S, Eloy JA. Laryngoscope. 2014;124:76–83. - PubMed
-
- Sinonasal carcinoma: clinical, pathological, genetic and therapeutic advances. Llorente JL, López F, Suárez C, Hermsen MA. Nat Rev Clin Oncol. 2014;11:460–472. - PubMed
-
- Prognostic factors and outcomes of de novo sinonasal squamous cell carcinoma: a systematic review and meta-analysis. Nguyen ES, Risbud A, Birkenbeuel JL, et al. Otolaryngol Head Neck Surg. 2022;166:434–443. - PubMed
-
- Squamous cell carcinoma and its variants. Mani N, Shah JP. Adv Otorhinolaryngol. 2020;84:124–136. - PubMed
Publication types
LinkOut - more resources
Full Text Sources