

Complete Versus Incomplete Revascularization in Elderly Patients With Myocardial Infarction: A Systematic Review and Meta-Analysis
- PMID: 39712780
- PMCID: PMC11660011
- DOI: 10.7759/cureus.74068
Complete Versus Incomplete Revascularization in Elderly Patients With Myocardial Infarction: A Systematic Review and Meta-Analysis
Abstract
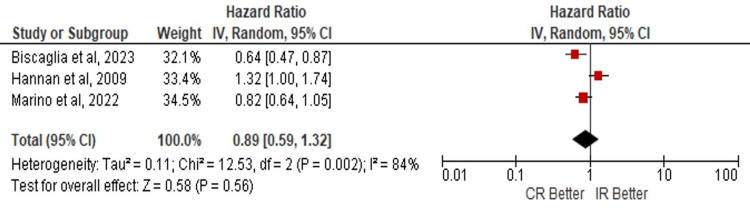
Coronary artery disease (CAD) is the leading cause of mortality in the United States, and percutaneous coronary intervention (PCI) is established as the standard after an acute episode of CAD. This review assessed the use of complete revascularization (CR) or incomplete revascularization (IR) in older adults, who present a higher cardiovascular risk. The aim is to define the effectiveness of both procedures in this population, focusing on major adverse cardiovascular events (MACE), myocardial infarction (MI), and all-cause mortality (ACM). A literature search identified 15 studies, evaluated using the Risk of Bias 2 (RoB 2) tool and the Risk of Bias in Non-Randomized Studies of Interventions I (ROBINS-I) tool for bias risk. Despite positive results in recent studies, this meta-analysis does not show the superiority of CR, demonstrating a lack of benefit in reducing mortality, myocardial infarction, and adverse events in the ≥ 70-year-old age group.
Keywords: coronary artery disease; coronary revascularization; major adverse cardiovascular events; myocardial infarction; older adults.
Copyright © 2024, Intriago et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures






Similar articles
-
Outcomes after complete versus incomplete revascularization of patients with multivessel coronary artery disease: a meta-analysis of 89,883 patients enrolled in randomized clinical trials and observational studies.J Am Coll Cardiol. 2013 Oct 15;62(16):1421-31. doi: 10.1016/j.jacc.2013.05.033. Epub 2013 Jun 7. J Am Coll Cardiol. 2013. PMID: 23747787
-
Clinical impact of complete revascularization in elderly patients with multi-vessel coronary artery disease undergoing percutaneous coronary intervention: A sub-analysis of the SHINANO registry.Int J Cardiol. 2017 Mar 1;230:413-419. doi: 10.1016/j.ijcard.2016.12.093. Epub 2016 Dec 21. Int J Cardiol. 2017. PMID: 28040276
-
Complete versus culprit-only percutaneous coronary intervention in elderly patients with acute coronary syndrome and multivessel coronary artery disease: A systematic review and meta-analysis.Cardiovasc Revasc Med. 2025 Jan;70:1-9. doi: 10.1016/j.carrev.2024.05.040. Epub 2024 Jun 1. Cardiovasc Revasc Med. 2025. PMID: 38849266
-
Intravascular ultrasound to guide percutaneous coronary interventions: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(12):1-97. Epub 2006 Apr 1. Ont Health Technol Assess Ser. 2006. PMID: 23074482 Free PMC article.
-
Impact of Complete or Incomplete Revascularization for Left Main Coronary Disease: The Extended PRECOMBAT Study.JACC Asia. 2023 Jan 24;3(1):65-74. doi: 10.1016/j.jacasi.2022.10.007. eCollection 2023 Feb. JACC Asia. 2023. PMID: 36873760 Free PMC article.
References
-
- Screening for coronary artery disease in patients with family history… how, when, and in whom? Blankstein R, Foody JM. Circ Cardiovasc Imaging. 2014;7:417–419. - PubMed
-
- Epidemiology and the magnitude of coronary artery disease and acute coronary syndrome: a narrative review. Ralapanawa U, Sivakanesan R. https://doi.org/10.2991/jegh.k.201217.001. J Epidemiol Glob Health. 2021;11:169–177. - PMC - PubMed
-
- Complete or culprit-only PCI in older patients with myocardial infarction. Biscaglia S, Guiducci V, Escaned J, et al. https://doi.org/10.1056/NEJMoa2300468. N Engl J Med. 2023;389:889–898. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous