

Digital mapping of resected cancer specimens: The visual pathology report
- PMID: 39712976
- PMCID: PMC11662268
- DOI: 10.1016/j.jpi.2024.100399
Digital mapping of resected cancer specimens: The visual pathology report
Abstract
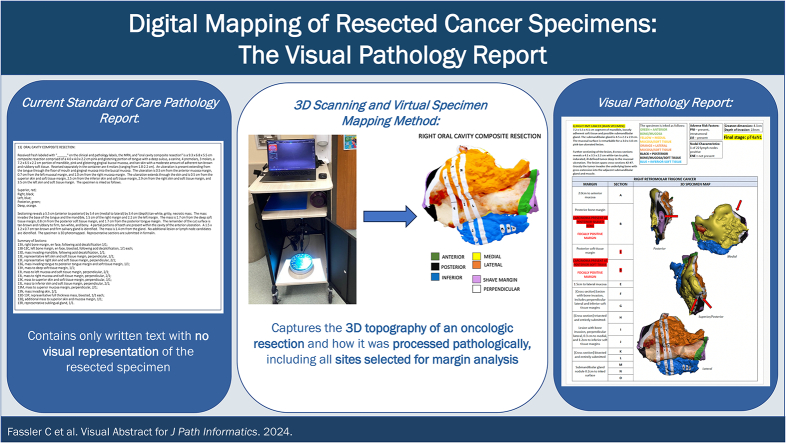
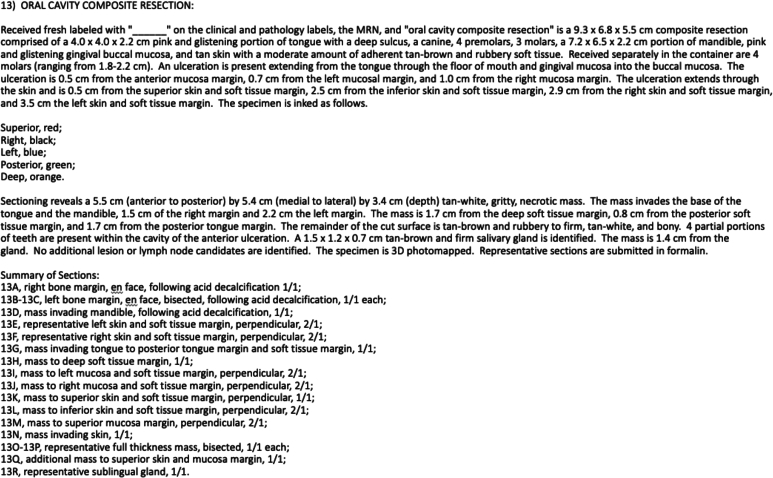
Background: The current standard-of-care pathology report relies only on lengthy written text descriptions without a visual representation of the resected cancer specimen. This study demonstrates the feasibility of incorporating virtual, three-dimensional (3D) visual pathology reports to improve communication of final pathology reporting.
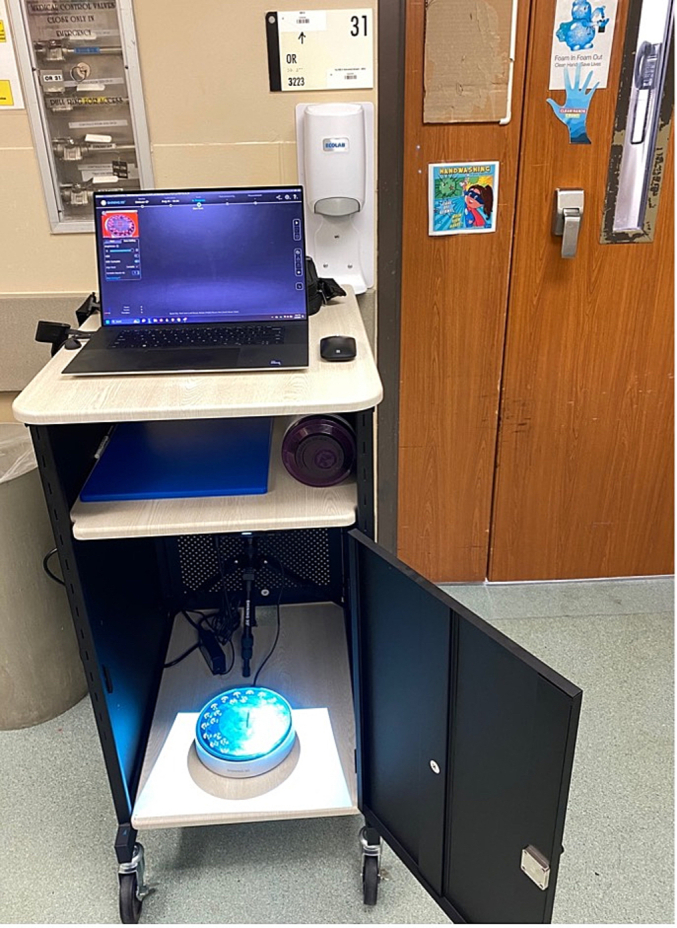
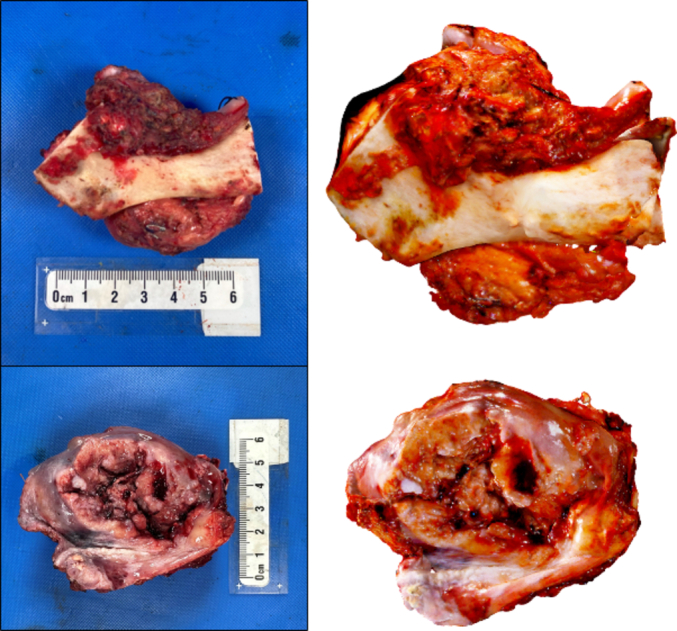
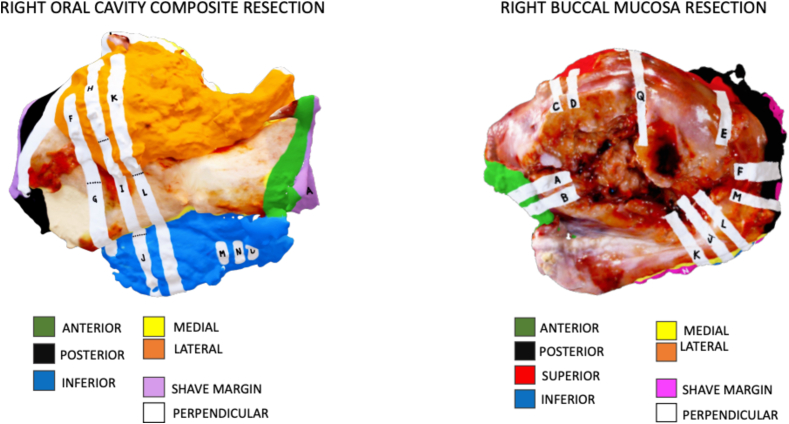
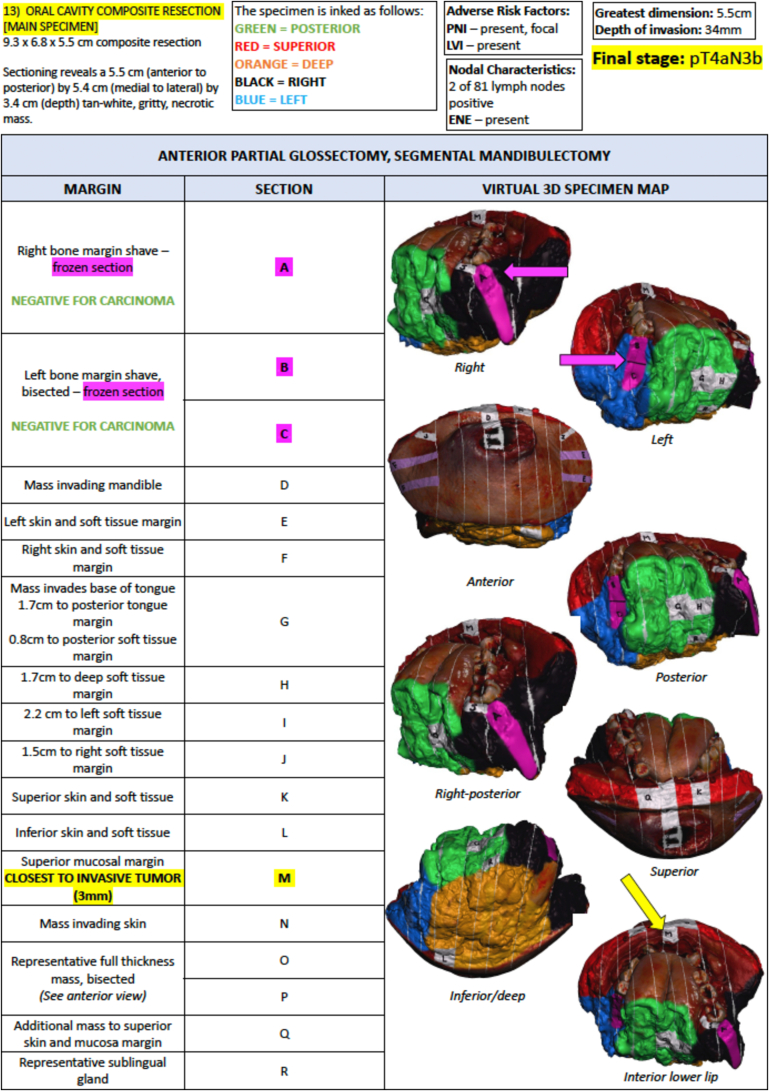
Materials and methods: Surgical specimens are 3D scanned and virtually mapped alongside the pathology team to replicate grossing. The 3D specimen maps are incorporated into a hybrid visual pathology report which displays the resected specimen and sampled margins alongside gross measurements, tumor characteristics, and microscopic diagnoses.
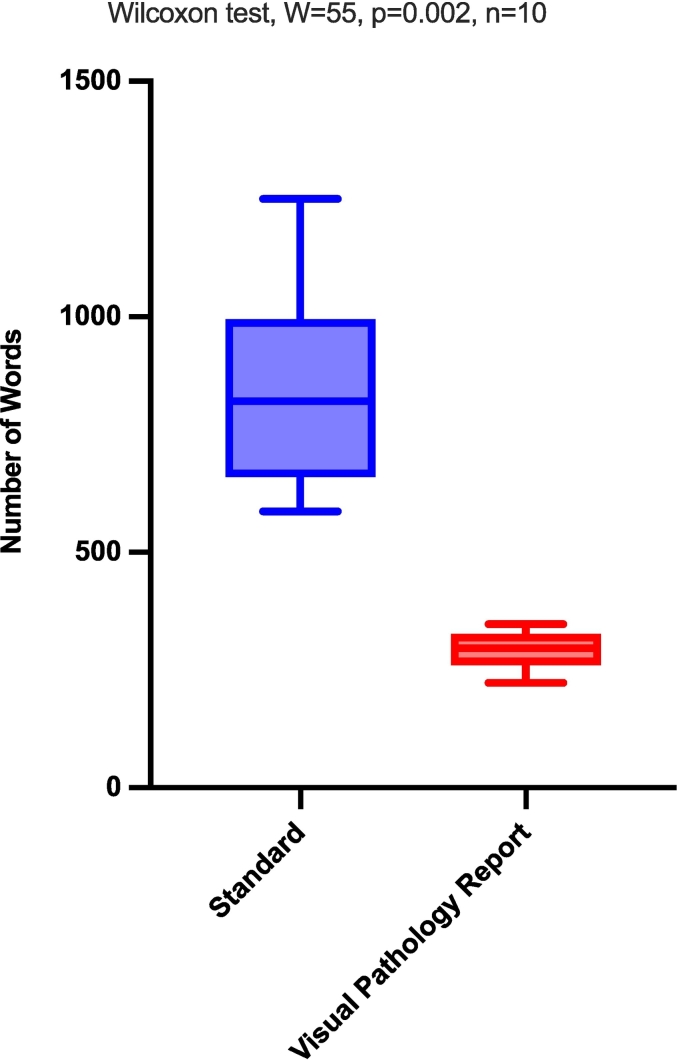
Results: Visual pathology reports were created for 10 head and neck cancer cases. Each report concisely communicated information from the final pathology report in a single page and contained significantly fewer words (293.4 words) than standard written pathology reports (850.1 words, p < 0.01).
Conclusions: We establish the feasibility of a novel visual pathology report that includes an annotated visual model of the resected cancer specimen in place of lengthy written text of standard of care head and neck cancer pathology reports.
Keywords: 3D scanning; Head and neck cancer; Margin status; Oral cavity cancer; Pathology communication; Virtual mapping.
© 2024 The Author(s).
Figures
References
-
- Network N.C.C. Head and Neck Cancers (Version 2.2024) https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf Updated 01/09/2024.
Grants and funding
LinkOut - more resources
Full Text Sources
