

Percutaneous closure of veno-venous collaterals in adult patients with univentricular physiology after Fontan palliation: Single centre experience and systematic review
- PMID: 39712986
- PMCID: PMC11657254
- DOI: 10.1016/j.ijcchd.2023.100479
Percutaneous closure of veno-venous collaterals in adult patients with univentricular physiology after Fontan palliation: Single centre experience and systematic review
Abstract
Background: The Fontan operation resulted in improved survival of patients with congenital heart defects not equipped to sustain biventricular circulation. Long-term complications are common, such as veno-venous collaterals (VVC). The aim of this study was to evaluate patient characteristics, percutaneous treatment strategy and (short-term) outcomes in adult Fontan patients with VVC, and review literature to date.
Methods: In this single-centre retrospective observational cohort study, patients who underwent percutaneous VVC closure between 2017 and 2023 were identified.
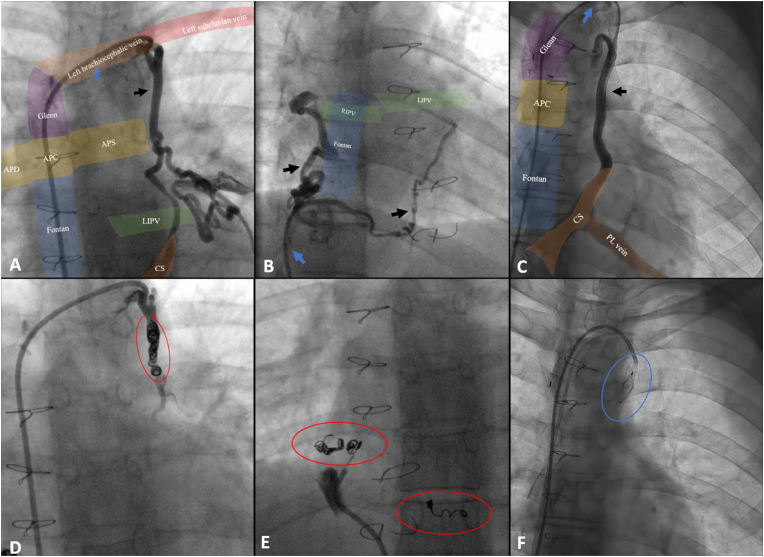
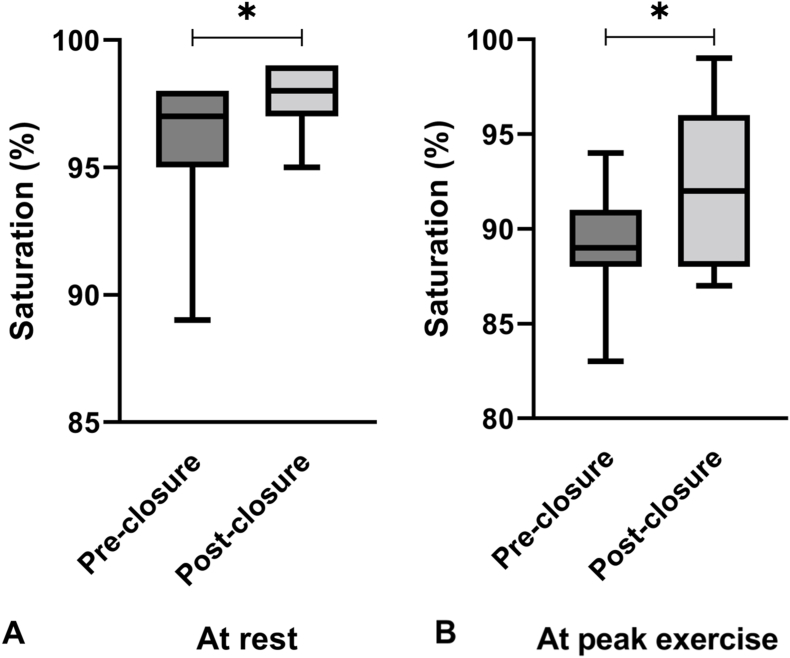
Results: Thirteen patients underwent percutaneous VVC closure (77 % female, age at intervention 24 ± 4 years, 77 % systemic left ventricle, 77 % extracardiac tunnel, median conduit size 16 [16-20]mm). Indications for closure were symptoms and/or significant exercise-related hypoxia. Mean Fontan pressure was 10±4 mmHg. The VVC originated from tributaries of the vena cava superior (VCS) and connected to pulmonary veins (8 VVC, 32 %), VCS to systemic atrium (3 VVC, 12 %), VCS to coronary sinus (3 VVC, 12 %) and tributaries of vena cava inferior to pulmonary veins (11 VVC, 44 %). Twenty-three VVC were occluded using coils and/or plugs. No periprocedural complications occurred. At first follow-up at least 6 months after closure (n = 11), 9 patients (82 %) reported symptom reduction. Saturation at rest and peak exercise increased significantly (96 ± 3 to 98 ± 1 %, p = 0.040; 89 ± 3 to 93 ± 5 %, p = 0.024, respectively). Exercise capacity remained unchanged.
Conclusions: VVC typically connect the tributaries of the vena cava inferior and/or superior with the pulmonary veins. Low Fontan pressures do not exclude the presence of VVC. Percutaneous closure of VVC is technically feasible, safe, and associated with symptom reduction and a significant rise in resting and exercise oxygen saturation.
Keywords: Adult congenital heart disease; Fontan circulation; Long term complications; Transcatheter interventions; Univentricular heart; Veno-venous collaterals.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures



Similar articles
-
Systemic to pulmonary venous collaterals in adults with single ventricle physiology after cavopulmonary palliation.Int J Cardiol. 2015 Jun 15;189:159-63. doi: 10.1016/j.ijcard.2015.04.065. Epub 2015 Apr 10. Int J Cardiol. 2015. PMID: 25897896
-
Modification of hemi-Fontan operation for patients with functional single ventricle and anomalous pulmonary venous connection to the superior vena cava: mid-term results.Interact Cardiovasc Thorac Surg. 2016 May;22(5):546-52. doi: 10.1093/icvts/ivv398. Epub 2016 Feb 8. Interact Cardiovasc Thorac Surg. 2016. PMID: 26860898 Free PMC article.
-
Percutaneous transcatheter closure of a large systemic to pulmonary venous fistulae in an adult patient after extracardiac fontan.Catheter Cardiovasc Interv. 2015 Sep;86(3):472-5. doi: 10.1002/ccd.25898. Epub 2015 Jul 21. Catheter Cardiovasc Interv. 2015. PMID: 25708733
-
Conversion of prior univentricular repairs to septated circulation: Case selection, challenges, and outcomes.Indian J Thorac Cardiovasc Surg. 2021 Jan;37(Suppl 1):91-103. doi: 10.1007/s12055-020-00938-9. Epub 2020 Jul 1. Indian J Thorac Cardiovasc Surg. 2021. PMID: 33603287 Free PMC article. Review.
-
Extracardiac Fontan operation without cardiopulmonary bypass.J Cardiovasc Surg (Torino). 2006 Dec;47(6):699-704. J Cardiovasc Surg (Torino). 2006. PMID: 17043618 Review.
References
-
- Rychik J., Atz A.M., Celermajer D.S., et al. Evaluation and management of the child and adult with fontan circulation: a scientific statement from the American heart association. Circulation. 2019 - PubMed
-
- Baumgartner H., De Backer J., Babu-Narayan S.V., et al. ESC Guidelines for the management of adult congenital heart disease. Eur Heart J 2021. 2020;42:563–645. - PubMed
LinkOut - more resources
Full Text Sources
