

Cognitive Behavioral Therapy Reduces Unhelpful Thinking Among People with Musculoskeletal Symptoms: A Meta-Analysis
- PMID: 39713097
- PMCID: PMC11660068
- DOI: 10.1177/24705470241304252
Cognitive Behavioral Therapy Reduces Unhelpful Thinking Among People with Musculoskeletal Symptoms: A Meta-Analysis
Abstract
Background: Greater unhelpful thinking is associated with greater musculoskeletal discomfort and incapability. Cognitive-behavioral therapy (CBT) fosters healthy thinking to help alleviate symptoms.
Questions: In a meta-analysis of randomized control trials (RCT) of CBT for unhelpful thinking among people with musculoskeletal symptoms, we asked: 1) Does CBT reduce unhelpful thinking and feelings of distress, and improve capability, in individuals with musculoskeletal symptoms? 2) Are outcomes affected by CBT delivery methods?
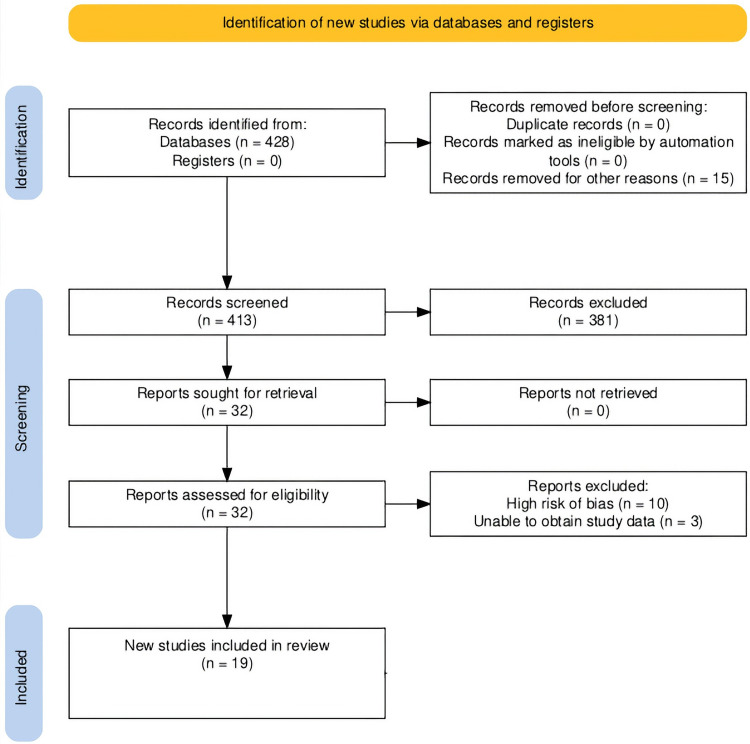
Methods: Following QUOROM guidelines, we searched databases using keywords of pain catastrophizing, kinesiophobia, cognitive-behavioral therapy, musculoskeletal and variations. Inclusion criteria were RCT's testing CBT among people with musculoskeletal symptoms. Study quality was assessed with Cochrane Review of Bias 2. Meta-analysis of means and standard deviations was performed.
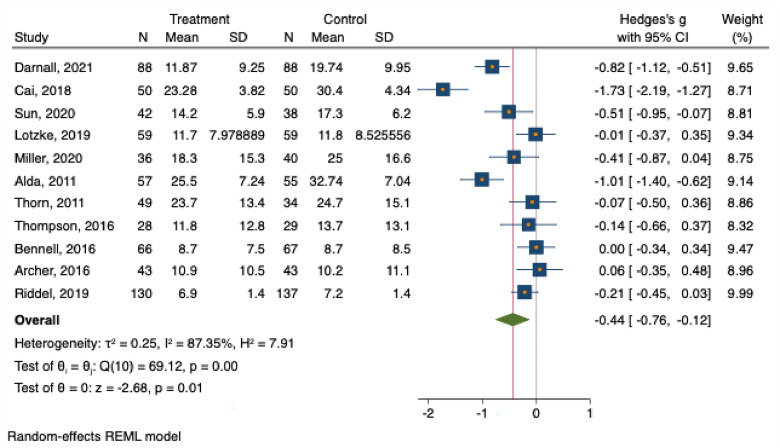
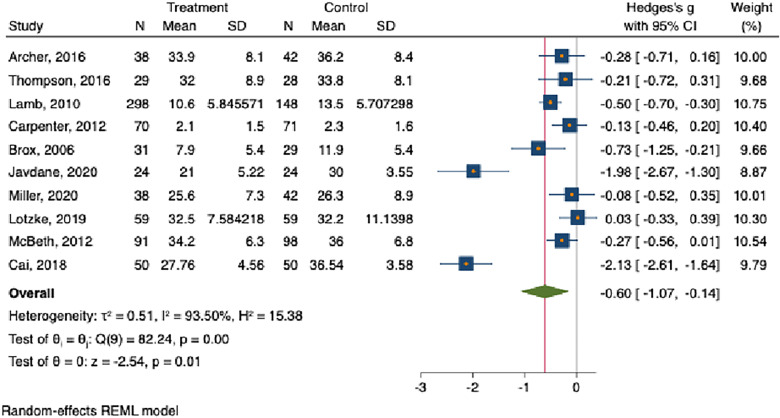
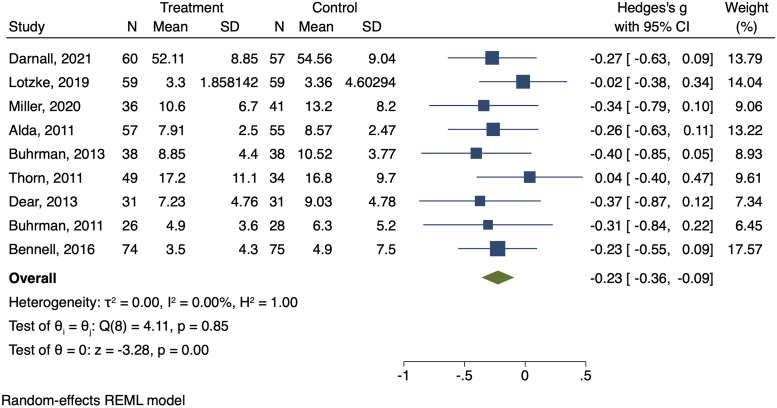
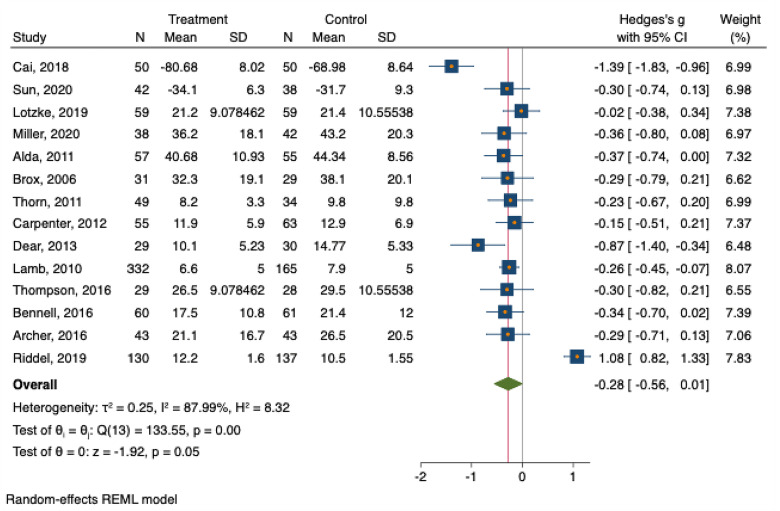
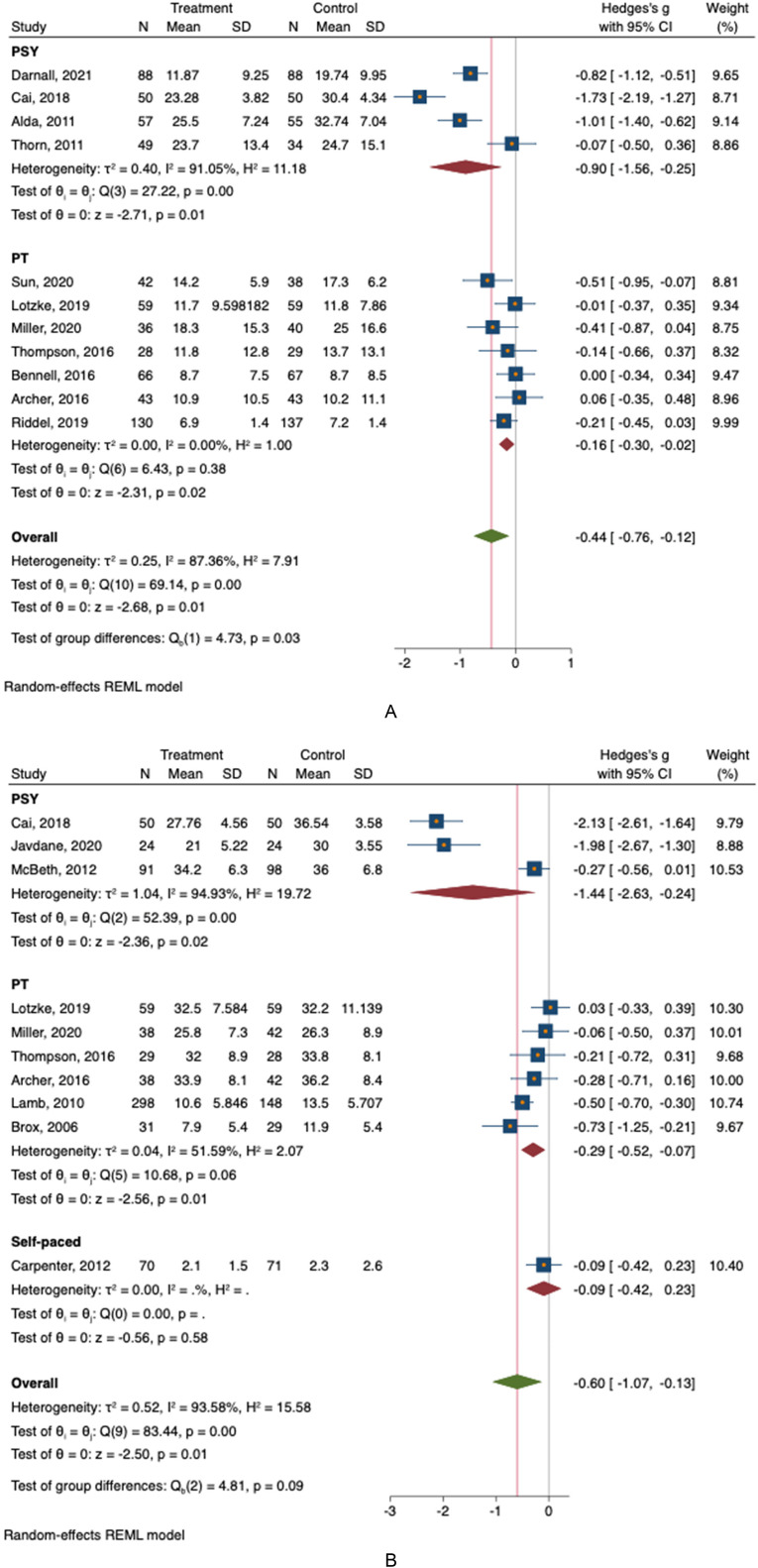
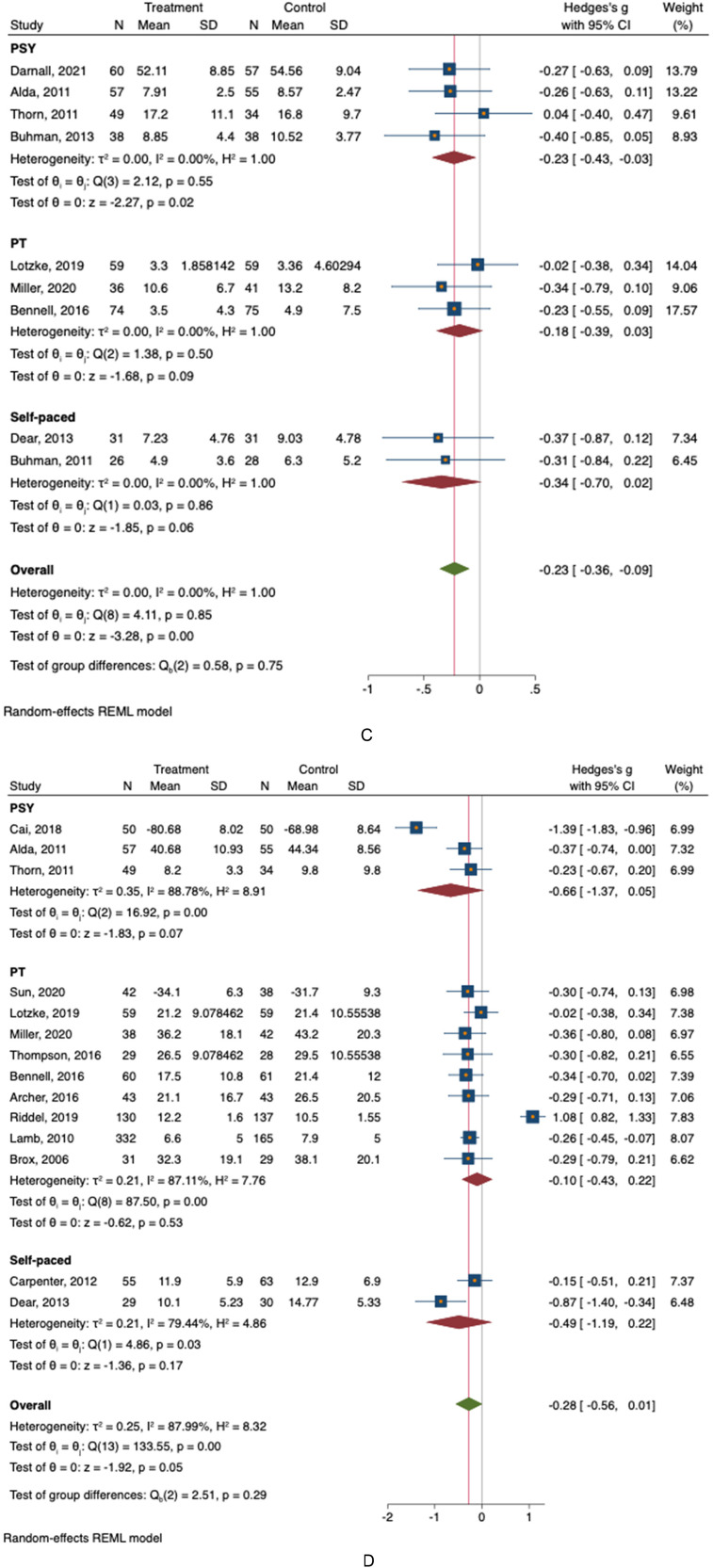
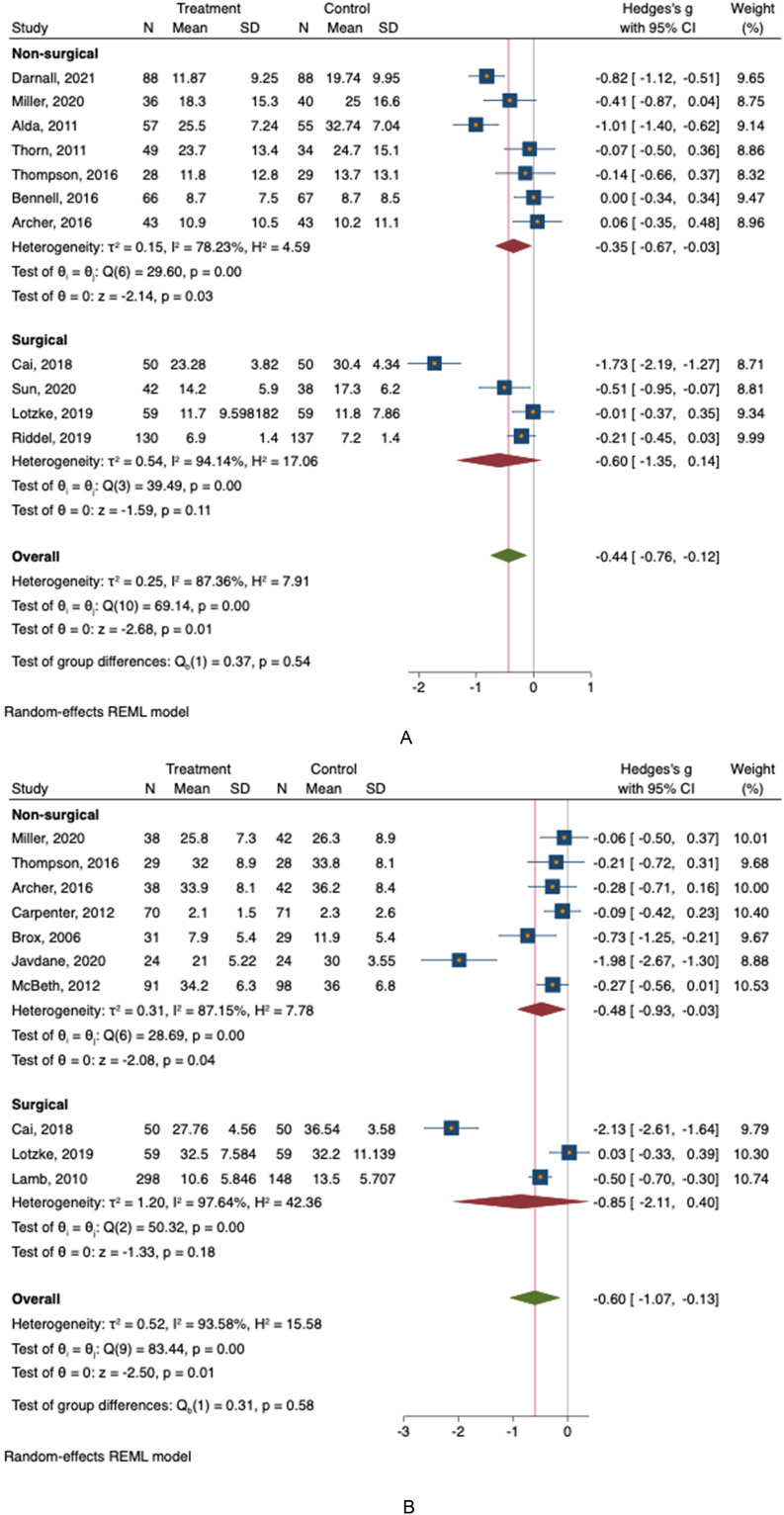
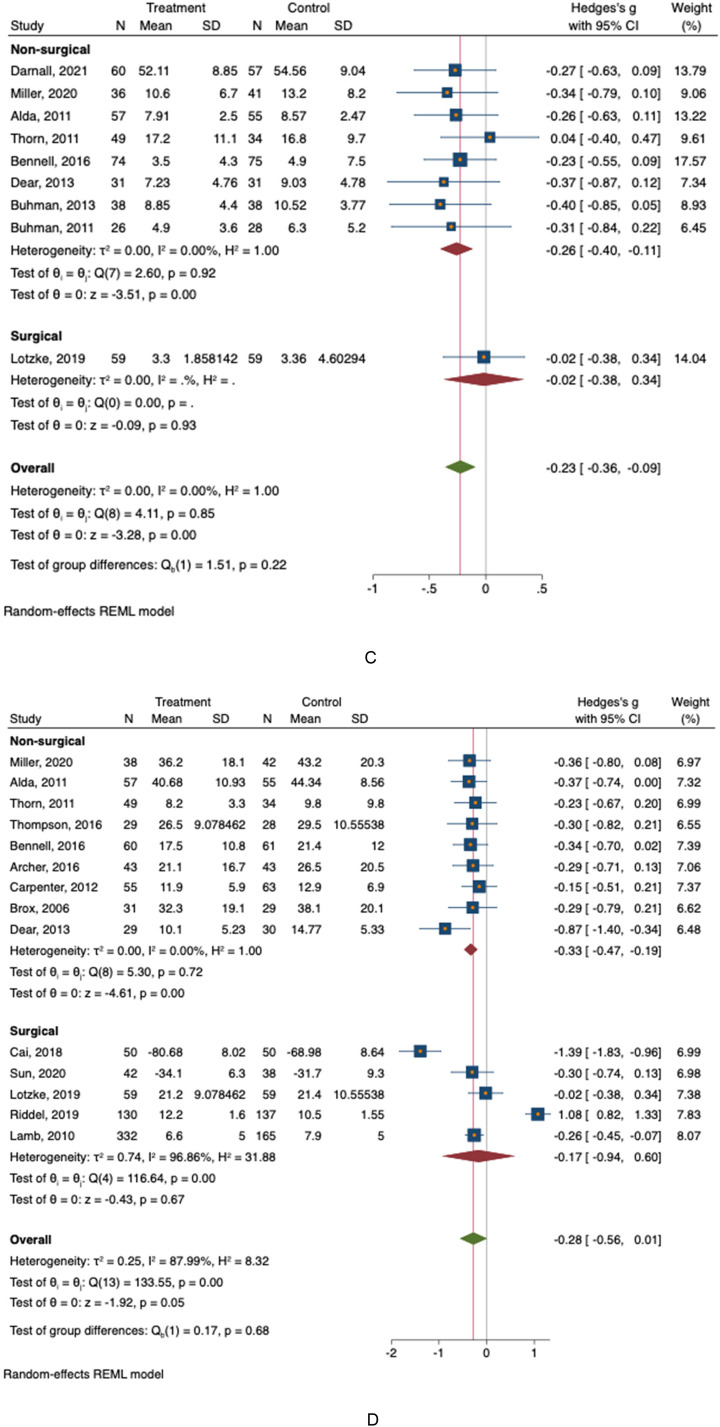
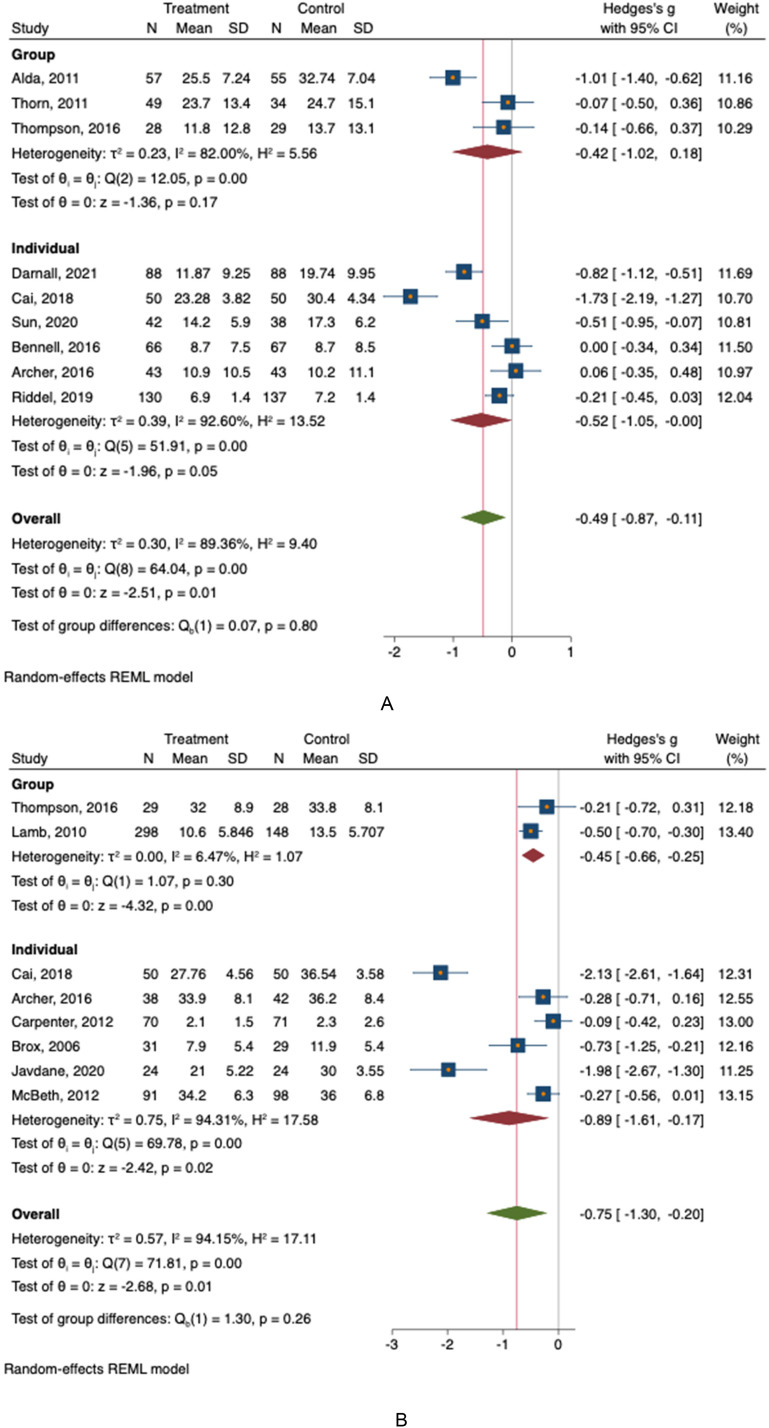
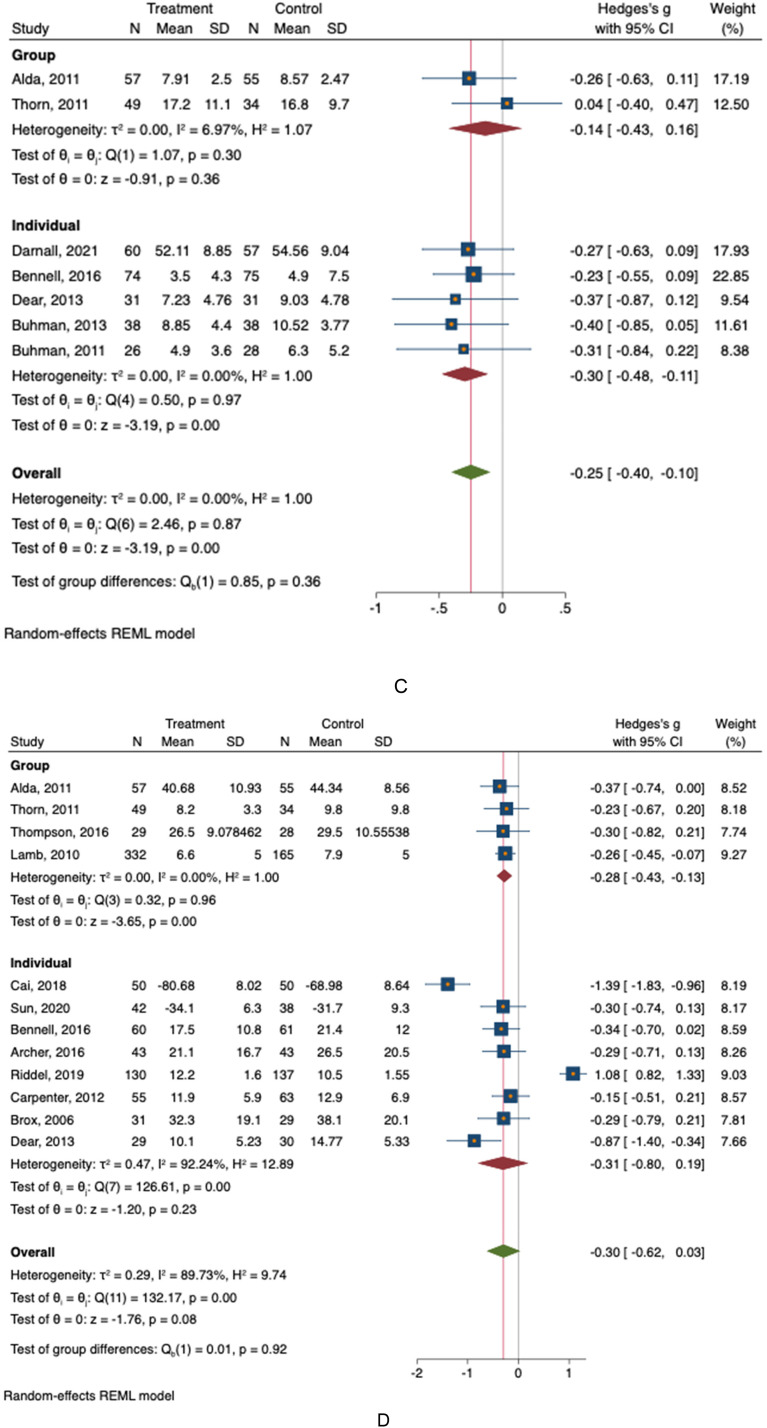
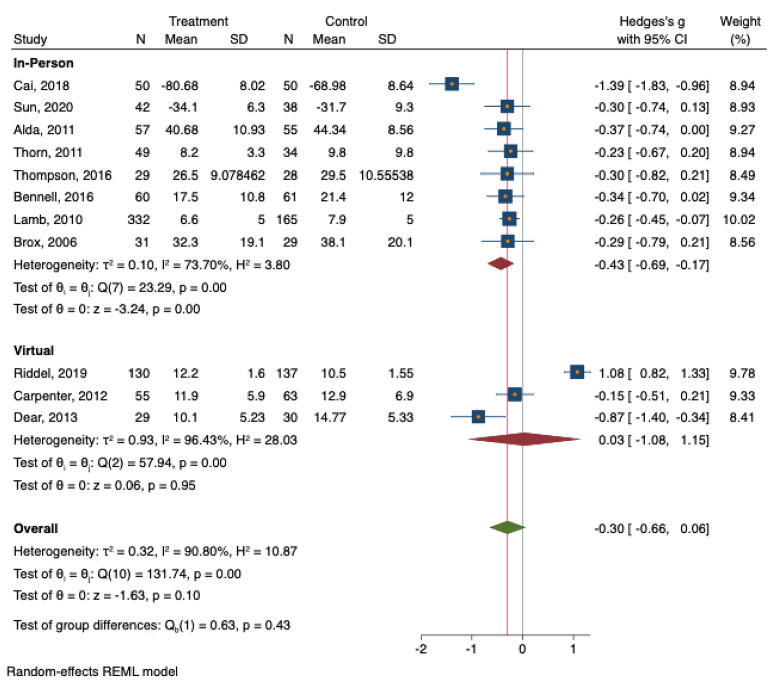
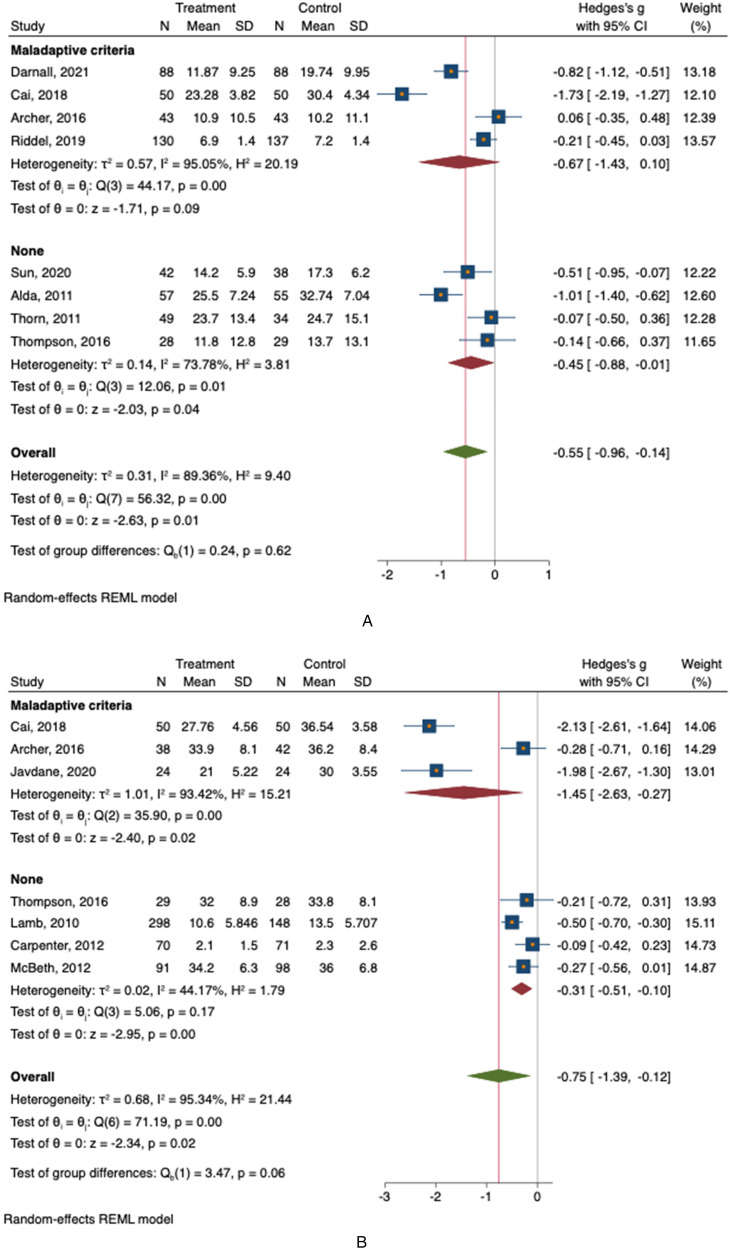
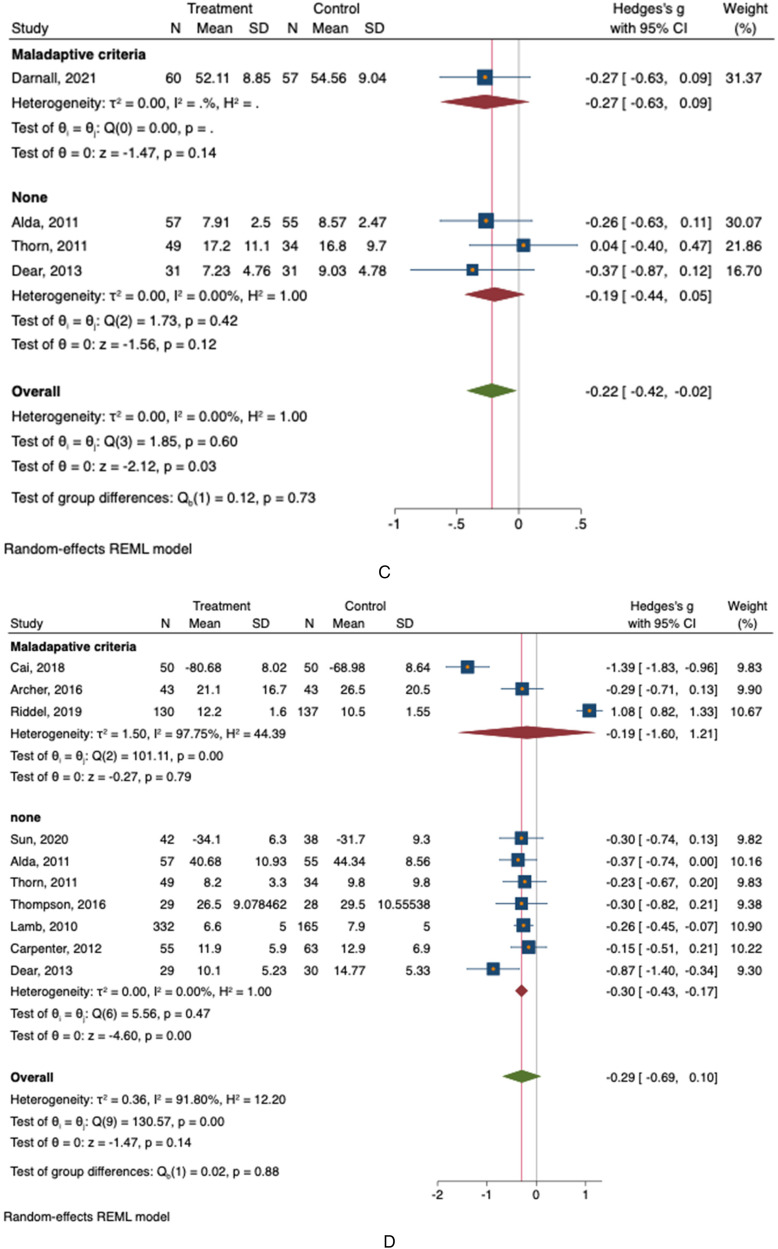
Results: CBT led to modest reductions in catastrophic thinking (-0.44 CI: -0.76 to -0.12; P = .01, kinesiophobia (-0.60 CI: -1.07 to -0.14; P = .01) and anxiety symptoms (-0.23 CI: -0.36 to -0.09; P < .01) over six months compared to usual care. There were no improvements in levels capability (-0.28 CI: -0.56 to 0.01; P = .05). CBT led by mental health professionals reduced catastrophic thinking more than CBT led by other clinicians (QB Test = 4.73 P = .03). There were no differences between online and in-person sessions, group versus individual therapy, or surgical versus non-surgical interventions.
Conclusion: The evidence that CBT delivered by various clinicians in various settings fosters healthier thinking in people presenting for care of musculoskeletal symptoms, supports comprehensive care of musculoskeletal illness. More research is needed to develop indications and interventions that also improve levels of capability. Level-I, meta-analysis of RCT's.
Keywords: anxiety symptoms; cognitive-behavioral therapy (CBT); fear avoidance; kinesiophobia; mental health interventions; pain catastrophizing; pain management; patient capability; recovery; unhelpful thinking.
© The Author(s) 2024.
Conflict of interest statement
Please separate ICMJE forms attached for each author details on conflicting interests.
Figures
Similar articles
-
Do Unhelpful Thoughts or Confidence in Problem Solving Have Stronger Associations with Musculoskeletal Illness?Clin Orthop Relat Res. 2022 Feb 1;480(2):287-295. doi: 10.1097/CORR.0000000000002005. Clin Orthop Relat Res. 2022. PMID: 34705738 Free PMC article.
-
Is Pain in the Uninjured Leg Associated With Unhelpful Thoughts and Distress Regarding Symptoms During Recovery From Lower Extremity Injury?Clin Orthop Relat Res. 2023 Dec 1;481(12):2368-2376. doi: 10.1097/CORR.0000000000002703. Epub 2023 May 29. Clin Orthop Relat Res. 2023. PMID: 37249315 Free PMC article.
-
Is Pain in the Uninjured Arm Associated With Unhelpful Thoughts and Distress Regarding Symptoms During Recovery From Upper-Extremity Injury?J Hand Surg Am. 2024 Dec;49(12):1266.e1-1266.e8. doi: 10.1016/j.jhsa.2023.03.019. Epub 2023 May 17. J Hand Surg Am. 2024. PMID: 37204359
-
Mobile apps to reduce depressive symptoms and alcohol use in youth: A systematic review and meta-analysis: A systematic review.Campbell Syst Rev. 2024 Apr 26;20(2):e1398. doi: 10.1002/cl2.1398. eCollection 2024 Jun. Campbell Syst Rev. 2024. PMID: 38680950 Free PMC article. Review.
-
A comparison of the effectiveness of cognitive behavioural interventions based on delivery features for elevated symptoms of depression in adolescents: A systematic review.Campbell Syst Rev. 2024 Jan 7;20(1):e1376. doi: 10.1002/cl2.1376. eCollection 2024 Mar. Campbell Syst Rev. 2024. PMID: 38188230 Free PMC article. Review.
References
-
- Archer KR, Wegener ST, Seebach C, et al. The effect of fear of movement beliefs on pain and disability after surgery for lumbar and cervical degenerative conditions. Spine (Phila Pa 1976). 2011. Sep;36(19): 1554–1562. - PubMed
-
- Browning RB, Clapp IM, Alter TD, Nwachukwu BU, Nho SJ. Pain catastrophizing and kinesiophobia affect return to sport in patients undergoing hip arthroscopy for the treatment of femoroacetabular impingement. Arthrosc Sports Med Rehabil [Internet]. 2021. Aug;3(4): e1087–e1095. Available from: 10.1016/j.asmr.2021.03.014 - DOI - PMC - PubMed
-
- Parrish JM, Jenkins NW, Parrish MS, et al. The influence of cognitive behavioral therapy on lumbar spine surgery outcomes: A systematic review and meta-analysis. Eur Spine J. 2021;30(5):1365–1379. Springer Science and Business Media Deutschland GmbH. - PubMed
LinkOut - more resources
Full Text Sources
