

Association Between the Albumin-Bilirubin (ALBI) Score and All-cause Mortality Risk in Intensive Care Unit Patients with Heart Failure
- PMID: 39713194
- PMCID: PMC11661052
- DOI: 10.5334/gh.1379
Association Between the Albumin-Bilirubin (ALBI) Score and All-cause Mortality Risk in Intensive Care Unit Patients with Heart Failure
Abstract
Background: The albumin-bilirubin (ALBI) score has demonstrated prognostic value in a range for liver and heart diseases. However, its association with all-cause mortality in intensive care unit (ICU) patients with heart failure remains uncertain.
Objective: This study sought to investigate the relationship between the ALBI score and the risk of all-cause mortality in ICU patients with heart failure.
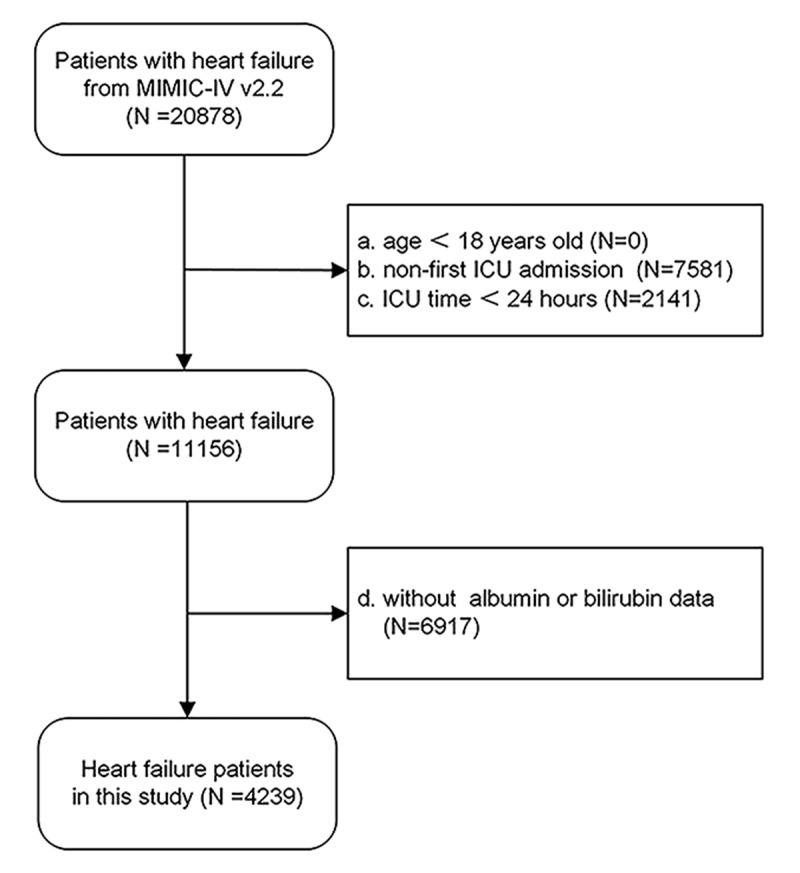
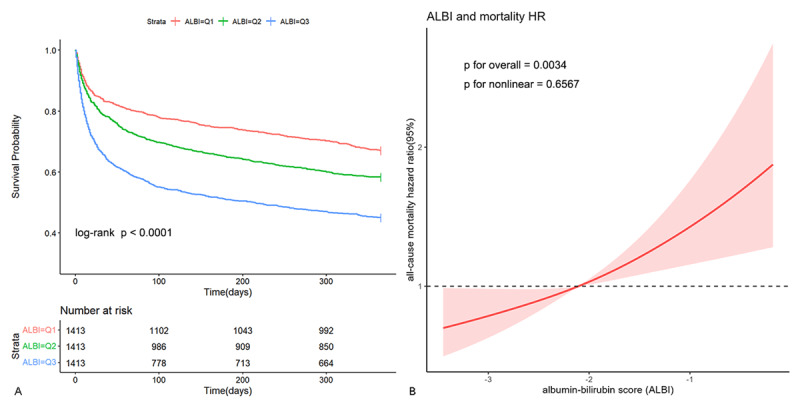
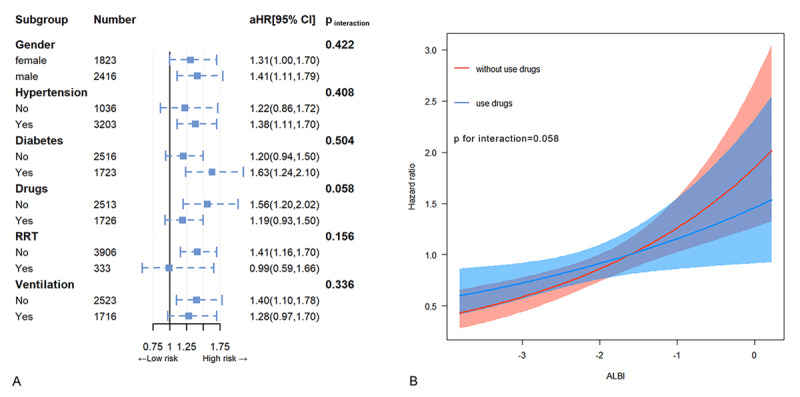
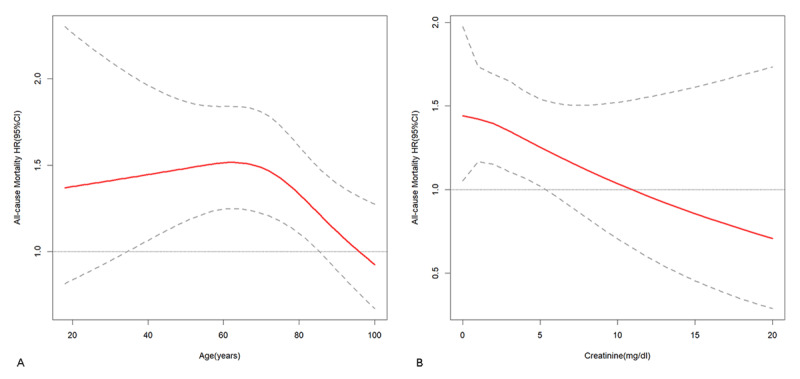
Methods and results: The ICU patients diagnosed with heart failure were selected from the Medical Information Mart for Intensive Care IV database (MIMIC-IV, version 2.2) and stratified into tertiles according to their ALBI scores. The primary outcome of interest was the occurrence of all-cause mortality within 365 days post-discharge. The analysis encompassed a cohort of 4,239 patients, with Kaplan-Meier curves indicating that individuals with higher ALBI levels exhibited an elevated risk of all-cause mortality (log-rank p < 0.001). Multivariate adjusted Cox regression and subgroup analysis demonstrated that individuals in T2 (hazard ratio (HR) 1.09, 95% CI 0.99-1.21) and T3 (HR 1.17, 95% CI 1.02-1.34) had an increased risk of mortality compared to individuals in T1 (p for trend < 0.001), and each incremental tertile in ALBI was linked to a 10% rise in mortality risk, while each individual unit increase in ALBI was associated with a 36% increase in mortality risk. This relationship was consistently observed across most subgroups, except for using or not using inotropes or vasopressors, different ages, different creatinine levels. The restricted cubic spline (RCS) analysis indicated a linear relationship between ALBI levels and the risk of all-cause mortality.
Conclusion: The ALBI scores are independently associated with the risk of all-cause mortality in ICU patients with heart failure, particularly in those not using inotropes or vasopressors, younger patients, and with lower levels of creatinine. ALBI may help identify high-risk patients and optimize risk stratification in this population.
Keywords: Albumin-bilirubin; Heart failure; Prognosis; intensive care unit; mortality.
Copyright: © 2024 The Author(s).
Conflict of interest statement
The authors have no competing interests to declare.
Figures
Similar articles
-
Association of albumin-bilirubin grade with short- and long-term mortality in patients with heart failure: a cohort study using restricted cubic splines and propensity score matching.BMC Cardiovasc Disord. 2025 Apr 23;25(1):307. doi: 10.1186/s12872-025-04760-2. BMC Cardiovasc Disord. 2025. PMID: 40269673 Free PMC article.
-
Independent prognostic importance of the albumin-corrected anion gap in critically ill patients with congestive heart failure: a retrospective study from MIMIC-IV database.BMC Cardiovasc Disord. 2024 Dec 20;24(1):735. doi: 10.1186/s12872-024-04422-9. BMC Cardiovasc Disord. 2024. PMID: 39707198 Free PMC article.
-
Prognostic value of the albumin-bilirubin score in critically ill patients with heart failure.Ann Palliat Med. 2021 Dec;10(12):12727-12741. doi: 10.21037/apm-21-3424. Ann Palliat Med. 2021. PMID: 35016474
-
Association between serum albumin creatinine ratio and all-cause mortality in intensive care unit patients with heart failure.Front Cardiovasc Med. 2024 Jul 4;11:1406294. doi: 10.3389/fcvm.2024.1406294. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39027002 Free PMC article.
-
Acute decompensated pulmonary hypertension outcomes in pulmonary arterial hypertension patients: systematic review and meta-analysis of proportions.Heart Lung. 2025 Mar-Apr;70:57-64. doi: 10.1016/j.hrtlng.2024.11.009. Epub 2024 Nov 23. Heart Lung. 2025. PMID: 39579648
Cited by
-
Development, Validation, and Deployment of a Time-Dependent Machine Learning Model for Predicting One-Year Mortality Risk in Critically Ill Patients with Heart Failure.Bioengineering (Basel). 2025 May 12;12(5):511. doi: 10.3390/bioengineering12050511. Bioengineering (Basel). 2025. PMID: 40428130 Free PMC article.
-
Predictive role of the Albumin-Bilirubin score in ICU patients with cirrhosis and sepsis: insights from a large retrospective cohort.BMC Gastroenterol. 2025 Jul 15;25(1):520. doi: 10.1186/s12876-025-04111-7. BMC Gastroenterol. 2025. PMID: 40665253 Free PMC article.
-
Association of albumin-bilirubin grade with short- and long-term mortality in patients with heart failure: a cohort study using restricted cubic splines and propensity score matching.BMC Cardiovasc Disord. 2025 Apr 23;25(1):307. doi: 10.1186/s12872-025-04760-2. BMC Cardiovasc Disord. 2025. PMID: 40269673 Free PMC article.
-
Independent prognostic importance of endothelial activation and stress index (EASIX) in critically ill patients with heart failure: modulating role of inflammation.Front Med (Lausanne). 2025 May 1;12:1560947. doi: 10.3389/fmed.2025.1560947. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40375932 Free PMC article.
References
-
- Harjola VP, Mullens W, Banaszewski M, Bauersachs J, Brunner-La Rocca HP, Chioncel O, et al. Organ dysfunction, injury and failure in acute heart failure: from pathophysiology to diagnosis and management. A review on behalf of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur J Heart Fail. 2017; 19:821–836. DOI: 10.1002/ejhf.872 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
