

Association between insurance type, clinical characteristics, and healthcare use in adults with congenital heart disease
- PMID: 39713233
- PMCID: PMC11657715
- DOI: 10.1016/j.ijcchd.2024.100543
Association between insurance type, clinical characteristics, and healthcare use in adults with congenital heart disease
Abstract
Introduction: Adults with congenital heart disease (CHD) represent a heterogeneous and growing population with high healthcare utilization. We sought to understand the association between insurance type, healthcare use, and outcomes among adults with CHD in Oregon.
Methods: The Oregon All Payers All Claims database from 2010 to 2017 was queried for adults aged 18-65 in 2014 with ICD-9 or 10 codes consistent with CHD; patient demographics, comorbidities, healthcare use, and disease severity were identified. Insurance type was categorized as either public (Medicare and Medicaid) or private (commercial). Descriptive statistics were used to compare groups. Use rates and odds ratios were calculated representing probability of at least one event per person-year using logistic regression with clustering on patients.
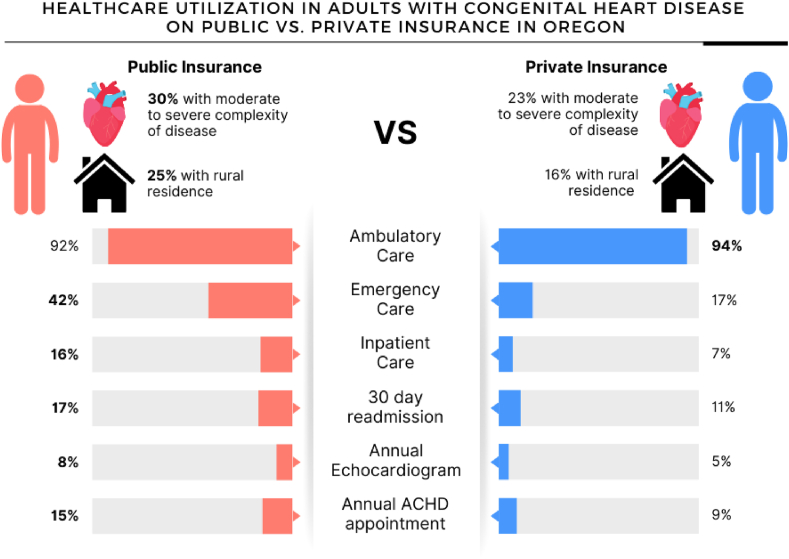
Results: Of 13,792 adults with CHD, 48 % had a form of public insurance. More publicly insured patients had moderate or severe anatomic complexity (29.5 % vs. 23.0 %; p < 0.0001), treatment for drug and alcohol use (25.0 % vs. 7.2 %; p < 0.0001), and mental health diagnoses (66.6 % vs. 51.0 %; p < 0.0001). They were more likely to reside in a rural area (24.5 % vs. 16.1 %; p < 0.0001). Adjusted for age and CHD severity, publicly insured patients were less likely to access overall ambulatory care (aOR 0.72, 99 % CI 0.66 to 0.80) but more likely to access emergency (aOR 3.86, 99 % CI 3.62 to 4.12) and inpatient (aOR 3.06, 99 % CI 2.81 to 3.33) care, as shown in Fig. 1. Length of hospital stay (5.7 vs. 4.4 days, p < 0.0001) and rates of 30-day readmission (17.1 % vs. 11.0 %, p < 0.001) were higher in those with public insurance. However, individuals with public insurance were significantly more likely to undergo their annual guideline-indicated echocardiogram (aOR 1.49, 99 % CI 1.23 to 1.80) and attend their annual ACHD visits (aOR 1.62, 99 % CI 1.40 to 1.87).
Conclusions: Our study shows that publicly insured adults with CHD in Oregon have more anatomically complex disease, more comorbidities, and higher healthcare use. While they were more likely to receive guideline-indicated ACHD care, they were also higher utilizers of emergency room and inpatient resources, implying that they may benefit from targeted interventions to improve outcomes and decrease unplanned healthcare use.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Stout K.K., et al. 2018 AHA/ACC guideline for the management of adults with congenital heart disease: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Circulation. 2019;139(14):e698–e800. - PubMed
LinkOut - more resources
Full Text Sources
