

Patterns and predictors of multiple sclerosis phenotype transition
- PMID: 39713244
- PMCID: PMC11660925
- DOI: 10.1093/braincomms/fcae422
Patterns and predictors of multiple sclerosis phenotype transition
Abstract
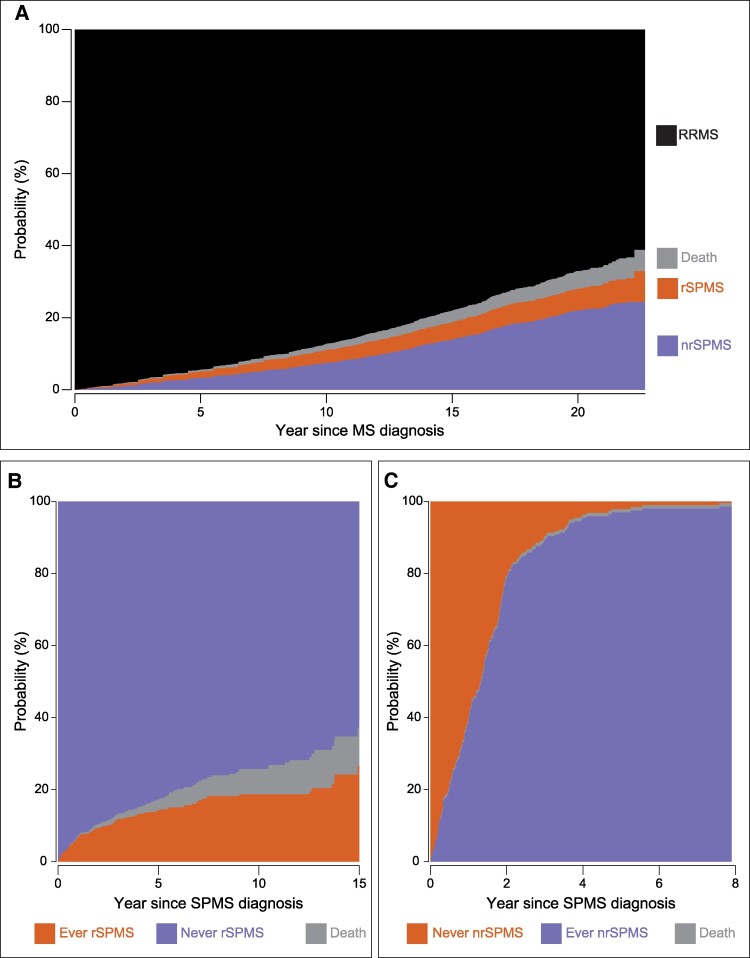
Currently, there are limited therapeutic options for patients with non-active secondary progressive multiple sclerosis. Therefore, real-world studies have investigated differences between patients with relapsing-remitting multiple sclerosis, non-active secondary progressive multiple sclerosis and active secondary progressive multiple sclerosis. Here, we explore patterns and predictors of transitioning between these phenotypes. We performed a cohort study using data from The Danish Multiple Sclerosis Registry. We included patients with a relapsing-remitting phenotype, registered changes to secondary progressive multiple sclerosis and subsequent transitions between relapsing and non-relapsing secondary progressive multiple sclerosis, which was defined by the presence of relapses in the previous 2 years. We analysed predictors of transitioning from relapsing-remitting multiple sclerosis to relapsing and non-relapsing secondary progressive multiple sclerosis, as well as between the secondary progressive states using a multi-state Markov model. We included 4413 patients with relapsing-remitting multiple sclerosis. Within a median follow-up of 16.2 years, 962 were diagnosed with secondary progressive multiple sclerosis by their treating physician. Of these, we classified 729 as non-relapsing and 233 as relapsing secondary progressive multiple sclerosis. The risk of transitioning from relapsing-remitting to non-relapsing secondary progressive multiple sclerosis included older age (hazard ratio per increase of 1 year in age: 1.044, 95% confidence interval: 1.035-1.053), male sex (hazard ratio for female: 0.735, 95% confidence interval: 0.619-0.874), fewer relapses (hazard ratio per each additional relapse: 0.863, 95% confidence interval: 0.823-0.906), higher expanded disability status scale (hazard ratio per each additional point: 1.522, 95% confidence interval: 1.458-1.590) and longer time on disease-modifying therapies (hazard ratio per increase of 1 year in treatment, high-efficacy disease-modifying therapy: 1.095, 95% confidence interval: 1.051-1.141; hazard ratio, moderate-efficacy disease-modifying therapy: 1.073, 95% confidence interval: 1.051-1.095). We did not find significant predictors associated with the transition from relapsing secondary progressive multiple sclerosis to non-relapsing secondary progressive multiple sclerosis, whereas older age (hazard ratio per increase of 1 year in age: 0.956, 95% confidence interval: 0.942-0.971) prevented the transition from non-relapsing secondary progressive multiple sclerosis to relapsing secondary progressive multiple sclerosis. Our study suggests that transitioning from relapsing-remitting multiple sclerosis to non-relapsing secondary progressive multiple sclerosis depends on well-known factors affecting diagnosing secondary progressive multiple sclerosis. Further transitions between non-relapsing and relapsing secondary progressive multiple sclerosis are only affected by age. These findings add to the knowledge of non-active secondary progressive multiple sclerosis, a patient group with unmet needs in terms of therapies.
Keywords: multiple sclerosis; real-world data; registry study; secondary progressive multiple sclerosis.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
N.G. and S.S.G. are employees of Sanofi and may hold shares and/or stock options in the company. M.F.W.-H. has served on the scientific advisory board for Sanofi and has received honoraria for lecturing for Novartis and Sanofi. H.B.J. has served as advisory board member for Merck and Roche and has received speaker honoraria from Biogen and Novartis. Z.I. has received speakers’ honoraria and/or research grants from Biogen, Roche, Sanofi, Novartis, Merck, Alexion, Bristol Myers Squibb, Lundbeckfonden, Jascha Fonden and Scleroseforeningen, has been member of advisory boards at Alexion, Biogen, Sanofi, Merck, Roche and Novartis, has been member of adjudication relapse (clinical endpoint) committees in Phase 3 trials and has been principal investigator in studies sponsored by Biogen, Merck and Sanofi. R.M.J. has served on scientific advisory boards for Novartis and Merck and has received conference travel support from Biogen. T.S. has served in scientific advisory board for Biogen, Merck, Novartis, Roche and Sanofi and has received honoraria for lecturing from Biogen, Merck, Novartis, Roche and Sanofi. A.W. has served on scientific advisory boards for Merck, Roche and Sanofi, has received conference travel support from Biogen, Merck, Roche, Sanofi and Novartis and speaker honoraria from Roche, Merck and Sanofi. M.R.M. has received support for participation in scientific meetings from Merck and Novartis, as well as travel grants from The Danish Multiple Sclerosis Society. M.B.P. has served on scientific advisory boards for Merck and support for conference participation from Novartis and Merck. S.P. received honoraria for contributing to making a magazine and support for congress participation from Merck. M.S. has served on scientific advisory boards for, received support for congress participation or received speaker honoraria from Biogen, Merck, Novartis, Roche and Sanofi Genzyme. P.V.R. has served on scientific advisory boards for, served as consultant for, received support for congress participation or received speaker honoraria from Alexion, Biogen, Bristol Myers Squibb, Merck, Novartis, Roche and Sanofi Genzyme. K.B.S. has served as consultant for Takeda, has received travel grants from TEVA, Biogen Merck and Novartis and has been principal investigator in studies sponsored by Alexion, Roche and Sanofi. F.S. has served on scientific advisory boards for, served as consultant for, received support for congress participation or received speaker honoraria from Alexion, Biogen, Bristol Myers Squibb, Lundbeck, Merck, Novartis, Roche and Sanofi Genzyme. His laboratory has received research support from Biogen, Merck, Novartis, Roche and Sanofi Genzyme. M.M. has served on scientific advisory boards, served as a consultant, received support for congress participation or received speaker honoraria from Roche, Sanofi, Biogen, Merck, Novartis, Bristol Myers Squibb, Medscape, Alexion and Moderna. Her research group has contracts with Biogen, Merck, Novartis, Roche, Sanofi and Bristol Myers Squibb. All other authors report no competing interests.
Figures



References
-
- Multiple Sclerosis International Federation—Atlas of MS . Accessed 2 May 2024. www.atlasofms.org
-
- Lublin FD, Reingold SC. Defining the clinical course of multiple sclerosis: Results of an international survey. National Multiple Sclerosis Society (USA) advisory committee on clinical trials of new agents in multiple sclerosis. Neurology. 1996;46(4):907–911. - PubMed
-
- Fambiatos A, Jokubaitis V, Horakova D, et al. Risk of secondary progressive multiple sclerosis: A longitudinal study. Mult Scler J. 2020;26(1):79–90. - PubMed
-
- Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17(2):162–173. - PubMed
LinkOut - more resources
Full Text Sources