

Surgical pulmonary valve replacement at a tertiary adult congenital heart centre in the current era
- PMID: 39713550
- PMCID: PMC11657547
- DOI: 10.1016/j.ijcchd.2022.100394
Surgical pulmonary valve replacement at a tertiary adult congenital heart centre in the current era
Abstract
Background: Surgical pulmonary valve replacement (PVR) is the standard cardiac operation in adult patients with congenital heart disease (ACHD). We report recent experience at a large tertiary centre and examine the impact of prosthesis type on outcomes.
Methods: All surgical PVRs performed at our tertiary centre between January 2003 and December 2018 were included.
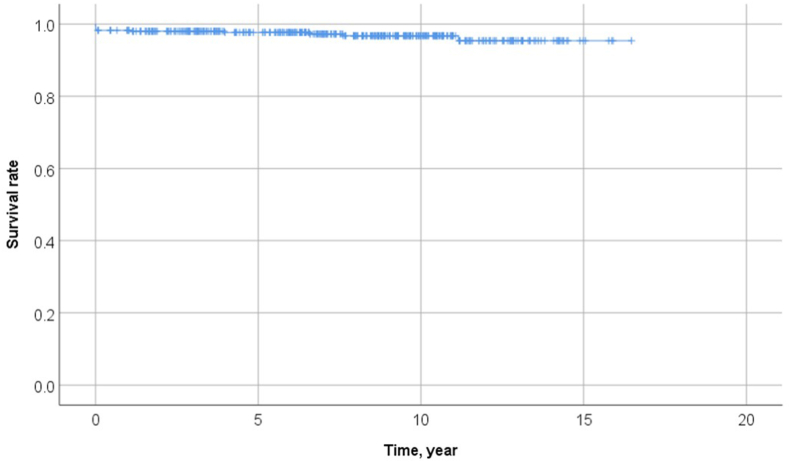
Results: The study population included 490 patients (197 women; mean age 29.9 ± 13 years). The types of valves used were Homograft 179 (37%), Perimount 152 (31%), Mosaic 120 (24%), Hancock 31 (6%), and others 5 (1%). Seven (1.4%) early deaths occurred within 30 days after surgery. The survival rates at 1, 5, 10, and 15 years of follow-up were 98.3%, 97.7%, 96.8%, and 95.4%, respectively, whereas freedom from re-intervention was 99.8%, 96.6%, 90.2%, and 81.0%, respectively. During a mean follow-up of 6.5 ± 4.3 years, 27 (5.5%) patients required re-intervention. The type of valve used in these 27 patients during index operation showed no discernible difference in the probability of re-intervention; however, Mosaic valves required earlier re-intervention compared to Perimount valves.
Conclusion: Our data show no discernible difference in reoperation rates between the different types of prostheses used. On-going surveillance of patients after PVR and further research in developing a life-long prosthesis are clearly warranted.
Keywords: Adult congenital heart disease; Pulmonary valve replacement; Tetralogy of fallot.
© 2022 The Authors.
Figures



Similar articles
-
Mid-term results of bioprosthetic pulmonary valve replacement in pulmonary regurgitation after tetralogy of Fallot repair.Eur J Cardiothorac Surg. 2012 Jul;42(1):e1-8. doi: 10.1093/ejcts/ezs219. Epub 2012 May 4. Eur J Cardiothorac Surg. 2012. PMID: 22561653
-
Long-term follow-up of homograft function after pulmonary valve replacement in patients with tetralogy of Fallot.Eur Heart J. 2006 Jun;27(12):1478-84. doi: 10.1093/eurheartj/ehl033. Epub 2006 May 17. Eur Heart J. 2006. PMID: 16707545
-
One hundred pulmonary valve replacements in children after relief of right ventricular outflow tract obstruction.Ann Thorac Surg. 2002 Jun;73(6):1801-6; discussion 1806-7. doi: 10.1016/s0003-4975(02)03568-3. Ann Thorac Surg. 2002. PMID: 12078772
-
Pulmonary valve replacement with a mechanical prosthesis. Promising results of 28 procedures in patients with congenital heart disease.Eur J Cardiothorac Surg. 2006 Jul;30(1):28-32. doi: 10.1016/j.ejcts.2006.02.069. Epub 2006 May 26. Eur J Cardiothorac Surg. 2006. PMID: 16730181 Review.
-
Current Readings: Issues Surrounding Pulmonary Valve Replacement in Repaired Tetralogy of Fallot.Semin Thorac Cardiovasc Surg. 2015 Spring;27(1):57-64. doi: 10.1053/j.semtcvs.2015.02.010. Epub 2015 Mar 7. Semin Thorac Cardiovasc Surg. 2015. PMID: 26074110 Review.
Cited by
-
Novel transparent patch as an adjunct to adult pulmonary valve replacement.Gen Thorac Cardiovasc Surg. 2025 May 11. doi: 10.1007/s11748-025-02154-x. Online ahead of print. Gen Thorac Cardiovasc Surg. 2025. PMID: 40349286
References
-
- Beurtheret S., Tutarel O., Diller G.P., et al. Contemporary cardiac surgery for adults with congenital heart disease. Heart (Br. Cardiac Soc.) 2017;103:1194–1202. - PubMed
-
- Ross D.N., Somerville J. Correction of pulmonary atresia with a homograft aortic valve. Lancet (London, England) 1966;2:1446–1447. - PubMed
-
- Frigiola A., Tsang V., Bull C., et al. Biventricular response after pulmonary valve replacement for right ventricular outflow tract dysfunction: is age a predictor of outcome? Circulation. 2008;118:S182–S190. - PubMed
-
- Buechel E.R., Dave H.H., Kellenberger C.J., et al. Remodelling of the right ventricle after early pulmonary valve replacement in children with repaired tetralogy of Fallot: assessment by cardiovascular magnetic resonance. Eur Heart J. 2005;26:2721–2727. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
