

Development and Validation of Nomograms to Predict the Overall Survival and Progression-Free Survival in Patients with Advanced Unresectable Intrahepatic Cholangiocarcinoma
- PMID: 39713568
- PMCID: PMC11663373
- DOI: 10.2147/CMAR.S489960
Development and Validation of Nomograms to Predict the Overall Survival and Progression-Free Survival in Patients with Advanced Unresectable Intrahepatic Cholangiocarcinoma
Abstract
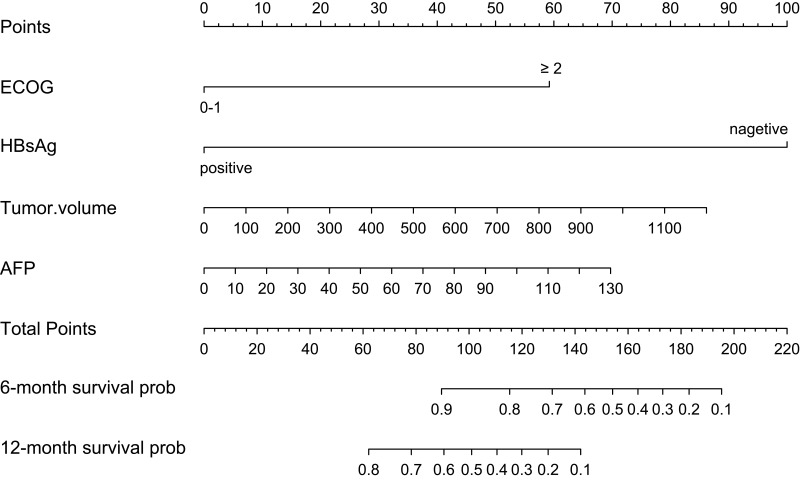
Purpose: This study aimed to develop and validate clinical nomograms for predicting progression-free survival (PFS) and overall survival (OS) in unresectable ICC patients.
Patients and methods: Patients with ICC between 1 January 2018 and 31 May 2023 were selected and randomized into a training set and an internal validation set as a 7:3 ratio. Data analysis and modeling were conducted through R software. The univariate and multivariate Cox regression models were used to analyze the prognosis factors affecting OS and PFS. Survival analysis was conducted using the Kaplan-Meier (KM) method, and comparisons were made using the Log rank test. Then, two nomogram models were constructed to predict OS and PFS, respectively. The nomogram was evaluated and calibrated using the Harrell's C-index, receiver operating characteristic curve (ROC), and calibration plots, and the decision curve analysis (DCA) was conducted to assess its clinical utility.
Results: A total of 110 patients were enrolled in this study, with 77 to the training set and 33 to the validation set. In the entire population, the OS rates at 6 and 12 months were 75.5% and 35.5%, respectively, while the PFS rates at 6 and 12 months were 47.3% and 20%, respectively. Cox regression analyses showed that ECOG, Tumor volume, HBsAg and AFP were the prognosis factors of OS, and the predictors in the model of PFS included Gender, Stage of tumor, CDC20 expression and AFP. The nomograms were constructed based on the predictors above. The C-index for predicting OS was 0.802 (0.755, 0.849) in the training set, 0.813 (0.764, 0.862) in the internal validation set; the C-index for predicting PFS was 0.658 (0.568, 0.748) in the training set, and 0.795 (0.705, 0.885) in the internal validation set. Finally, calibration curves and DCA indicated that two nomograms showed favorable performance.
Conclusion: Two practical and effective prognostic nomograms were developed to assist clinicians in evaluating OS and PFS in patients with unresectable ICC.
Keywords: intrahepatic cholangiocarcinoma; nomogram; overall survival; prognostic model; progression-free survival.
© 2024 Xian et al.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures







References
LinkOut - more resources
Full Text Sources
