

Plasma Aβ42/Aβ40 is sensitive to early cerebral amyloid accumulation and predicts risk of cognitive decline across the Alzheimer's disease spectrum
- PMID: 39713875
- PMCID: PMC11848181
- DOI: 10.1002/alz.14442
Plasma Aβ42/Aβ40 is sensitive to early cerebral amyloid accumulation and predicts risk of cognitive decline across the Alzheimer's disease spectrum
Abstract
Introduction: The availability of amyloid beta (Aβ) targeting therapies for Alzheimer's disease (AD) is increasing the demand for scalable biomarkers that are sensitive to early cerebral Aβ accumulation.
Methods: We evaluated fully-automated Lumipulse plasma Aβ42/Aβ40 immunoassays for detecting cerebral Aβ in 457 clinically unimpaired (CU) and clinically impaired (CI) Stanford Alzheimer's Disease Research Center (Stanford ADRC) participants and 186 CU in the Stanford Aging and Memory Study (SAMS). Longitudinal change in ADRC plasma Aβ42/Aβ40 and cognition and cross-sectional associations with SAMS memory and tau positron emission tomography (PET) were examined.
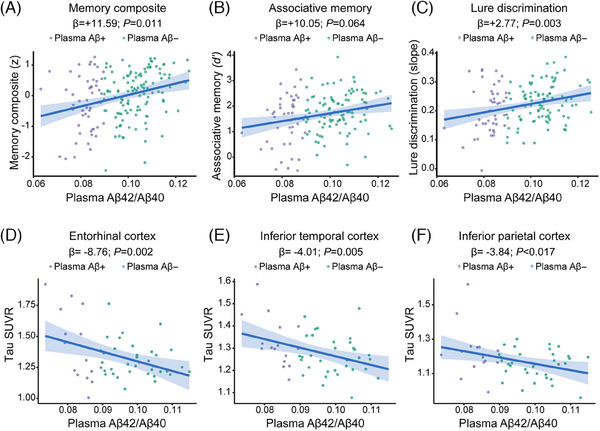
Results: Plasma Aβ42/Aβ40 exhibited high performance in detecting amyloid positivity defined by PET (area under the curve [AUC]: 0.885, 95% confidence interval [CI]: 0.816-0.955). Once abnomal, plasma Aβ42/Aβ40 remained low and predicted cognitive decline in both CU and CI individuals. Among SAMS CU, plasma Aβ42/Aβ40 was associated with poorer hippocampal-dependent memory and elevated tau accumulation.
Discussion: Lumipulse plasma Aβ42/Aβ40 is a scalable assay for detection of cerebral Aβ and prediction of risk for cognitive decline across the AD continuum.
Highlights: Lumipulse plasma amyloid beta (Aβ)42/Aβ40 exhibited high accuracy in detecting amyloid positivity. Plasma amyloid-positive (Aβ+) individuals exhibited stability of Aβ42/Aβ40 over time. Plasma Aβ42/Aβ40 predicted future cognitive decline across the Alzheimer's disease (AD) spectrum. Plasma Aβ42/Aβ40 was sensitive to memory and tau burden in clinically unimpaired older adults.
Keywords: Alzheimer's disease; blood biomarkers; cognition; plasma Aβ42/Aβ40.
© 2024 The Author(s). Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
The authors declare no conflicts of interest. Author disclosures are available in the supporting information.
Figures





Similar articles
-
Combining plasma Aβ and p-tau217 improves detection of brain amyloid in non-demented elderly.Alzheimers Res Ther. 2024 May 23;16(1):115. doi: 10.1186/s13195-024-01469-w. Alzheimers Res Ther. 2024. PMID: 38778353 Free PMC article.
-
Alzheimer's cerebrospinal biomarkers from Lumipulse fully automated immunoassay: concordance with amyloid-beta PET and manual immunoassay in Koreans : CSF AD biomarkers measured by Lumipulse in Koreans.Alzheimers Res Ther. 2021 Jan 12;13(1):22. doi: 10.1186/s13195-020-00767-3. Alzheimers Res Ther. 2021. PMID: 33436035 Free PMC article.
-
Performance of Plasma Biomarkers Combined with Structural MRI to Identify Candidate Participants for Alzheimer's Disease-Modifying Therapy.J Prev Alzheimers Dis. 2024;11(5):1198-1205. doi: 10.14283/jpad.2024.110. J Prev Alzheimers Dis. 2024. PMID: 39350364 Free PMC article.
-
Predictive Accuracy of Blood-Derived Biomarkers for Amyloid-β Brain Deposition Along with the Alzheimer's Disease Continuum: A Systematic Review.J Alzheimers Dis. 2021;84(1):393-407. doi: 10.3233/JAD-210496. J Alzheimers Dis. 2021. PMID: 34542072
-
Plasma Aβ as a biomarker for predicting Aβ-PET status in Alzheimer's disease:a systematic review with meta-analysis.J Neurol Neurosurg Psychiatry. 2022 May;93(5):513-520. doi: 10.1136/jnnp-2021-327864. Epub 2022 Mar 3. J Neurol Neurosurg Psychiatry. 2022. PMID: 35241627 Free PMC article.
Cited by
-
Synergistic effects of APOE ε4 and Alzheimer's pathology on the neural correlates of episodic remembering in cognitively unimpaired older adults.bioRxiv [Preprint]. 2025 Jun 25:2025.06.20.660774. doi: 10.1101/2025.06.20.660774. bioRxiv. 2025. PMID: 40667041 Free PMC article. Preprint.
-
Unveiling blood biomarkers for neuronal hyperplasticity: Insights from AD molecular subtyping, a comprehensive review.Alzheimers Dement. 2025 Jul;21(7):e70475. doi: 10.1002/alz.70475. Alzheimers Dement. 2025. PMID: 40709526 Free PMC article. Review.
-
Factor analysis of multimodal MRI, biofluid, and vascular biomarkers reveals latent constructs of brain health.Geroscience. 2025 Jul 8. doi: 10.1007/s11357-025-01771-x. Online ahead of print. Geroscience. 2025. PMID: 40627123
-
Parkinson's disease is characterized by vitamin B6-dependent inflammatory kynurenine pathway dysfunction.NPJ Parkinsons Dis. 2025 Apr 26;11(1):96. doi: 10.1038/s41531-025-00964-7. NPJ Parkinsons Dis. 2025. PMID: 40287426 Free PMC article.
References
MeSH terms
Substances
Grants and funding
- K99 AG075184/AG/NIA NIH HHS/United States
- U24 AG021886/AG/NIA NIH HHS/United States
- K99 AG071837/AG/NIA NIH HHS/United States
- K99AG071837/GF/NIH HHS/United States
- R01AG060747/GF/NIH HHS/United States
- K99AG075184/GF/NIH HHS/United States
- U24AG021886/National Centralized Repository Alzheimer's Disease and Related Dementias
- Scully Research Initiative
- P50 AG047366/AG/NIA NIH HHS/United States
- Stanford PHIND Institute
- Jean Perkins Foundation
- Good Planet Foundation
- P50AG047366/GF/NIH HHS/United States
- R01 AG048076/AG/NIA NIH HHS/United States
- R01 AG060747/AG/NIA NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- P30 AG066515/AG/NIA NIH HHS/United States
- R01AG074339/GF/NIH HHS/United States
- R01AG048076/GF/NIH HHS/United States
- The Phil and Penny Knight Initiative for Brain Resilience
- R35 AG072290/AG/NIA NIH HHS/United States
- P30AG066515/GF/NIH HHS/United States
- R01 AG074339/AG/NIA NIH HHS/United States
- AARFD-21-849349/ALZ/Alzheimer's Association/United States
- R35AG072290/GF/NIH HHS/United States
- U24AG021886/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
