

Restricting Periodontal Treatment Frequency: Impact on Tooth Loss in Danish Adults
- PMID: 39715711
- PMCID: PMC11892545
- DOI: 10.1111/cdoe.13022
Restricting Periodontal Treatment Frequency: Impact on Tooth Loss in Danish Adults
Abstract
Objective: The study aimed to estimate the effect of a periodontal treatment policy that would restrict the receipt of periodontal therapy to no more than once every second year, on the 10-year risk of tooth extraction among Danish adults.
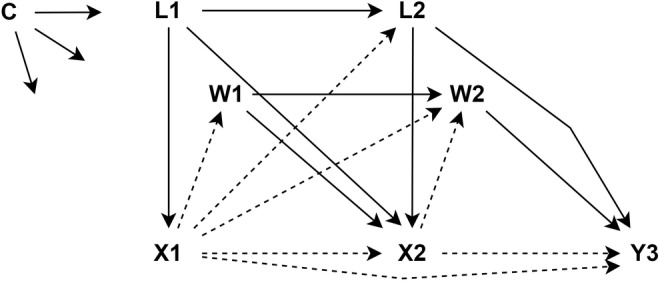
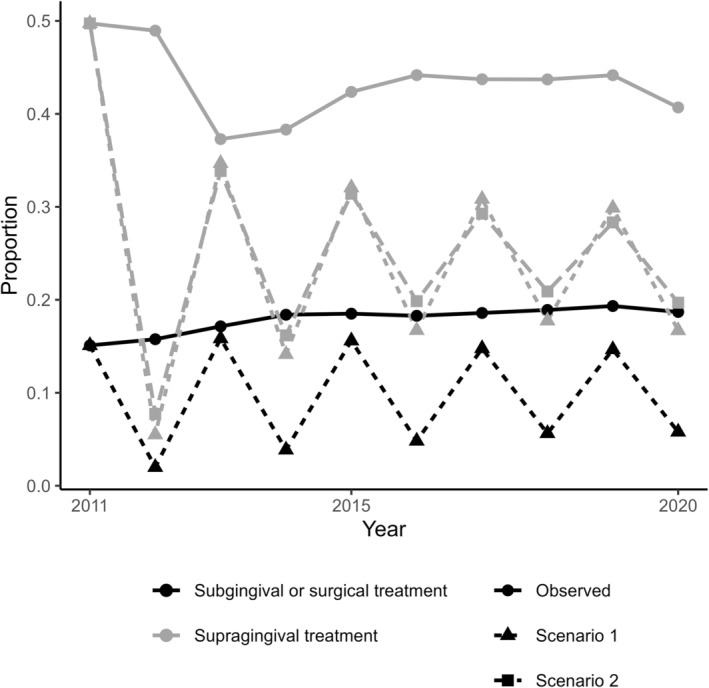
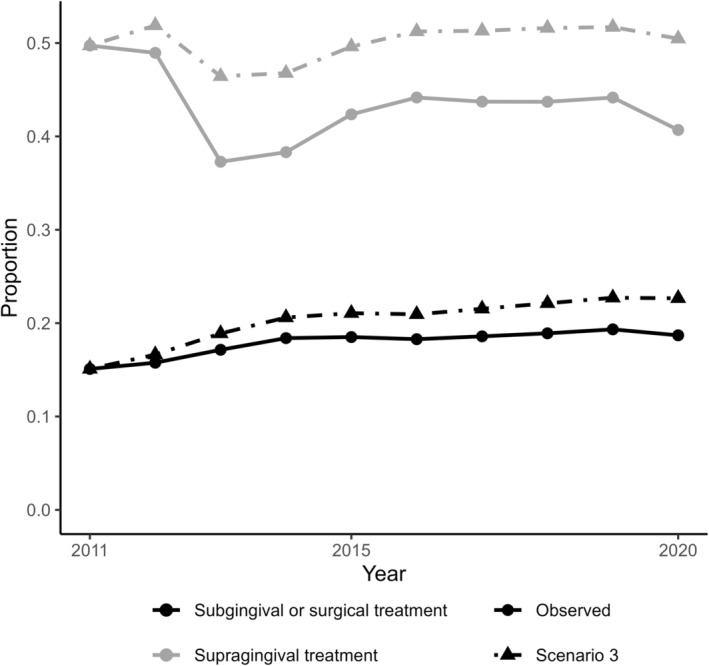
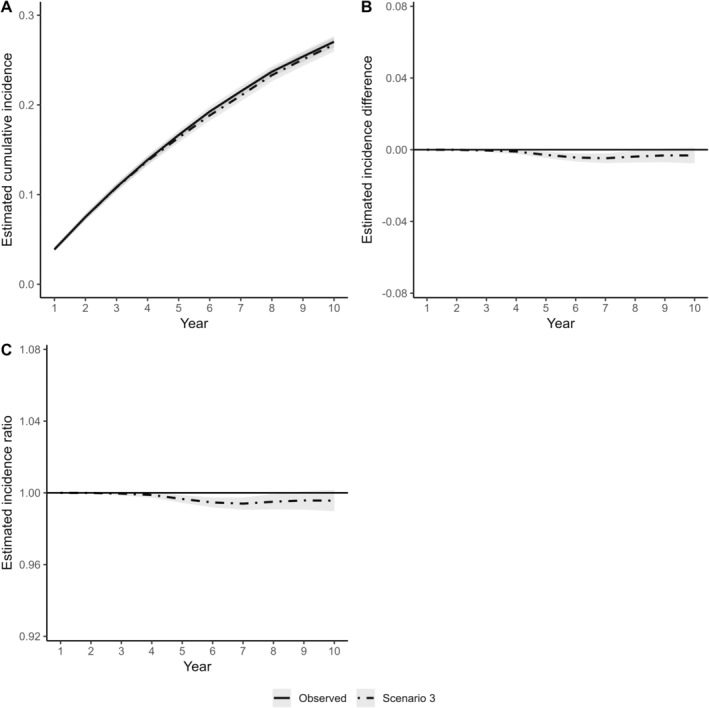
Methods: Data from linked nationwide Danish registers consisted of a random sample of 20 000 50-year-olds who were followed from the beginning of 1990 to the end of 2021. The longitudinal modified treatment policies' causal inference framework was used. In each of two slightly different counterfactual scenarios, the receipt of supragingival or subgingival periodontal therapy was restricted to no more than once every second year. The cumulative incidence of tooth extraction from 2012 to 2021 was compared between the counterfactual scenarios and the observed periodontal visiting pattern, while informative censoring, and time-varying and time-invariant confounding were accounted for using the social, economic and dental service utilisation history.
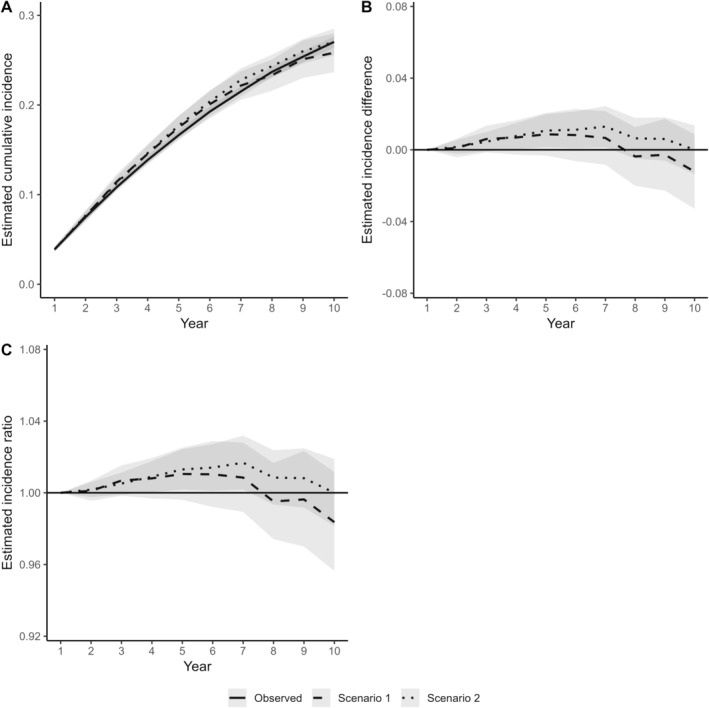
Results: During the 10-year follow-up period, 5021 (25.1%) individuals received at least one tooth extraction. In the two counterfactual scenarios, the number of years receiving supragingival or subgingival periodontal therapy was 30%-50% lower than in the observed data. The 10-year cumulative incidence of tooth loss was practically the same in the two counterfactual scenarios as under the observed periodontal visiting patterns.
Conclusion: The findings indicate that a considerable decrease in the number and frequency of periodontal care visits would not have significant impact on the incidence of tooth loss in Denmark.
Keywords: Dental services research; Epidemiology; Periodontitis; Public health policy; Statistics.
© 2024 The Author(s). Community Dentistry and Oral Epidemiology published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Chapple I. L., Van der Weijden F., Doerfer C., et al., “Primary Prevention of Periodontitis: Managing Gingivitis,” Journal of Clinical Periodontology 42, no. Suppl 16 (2015): S71–S76. - PubMed
-
- West N., Chapple I., Claydon N., et al., “BSP Implementation of European S3—Level Evidence‐Based Treatment Guidelines for Stage I–III Periodontitis in UK Clinical Practice,” Journal of Dentistry 106 (2021): 103562. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
