

Lymphatic plastic bronchitis: a study based on CT and MR lymphangiography
- PMID: 39716172
- PMCID: PMC11668086
- DOI: 10.1186/s12880-024-01504-0
Lymphatic plastic bronchitis: a study based on CT and MR lymphangiography
Abstract
Objectives: To investigate the diagnostic value of CT lymphangiography (CTL) and non-contrast MR lymphangiography (MRL) in lymphatic plastic bronchitis.
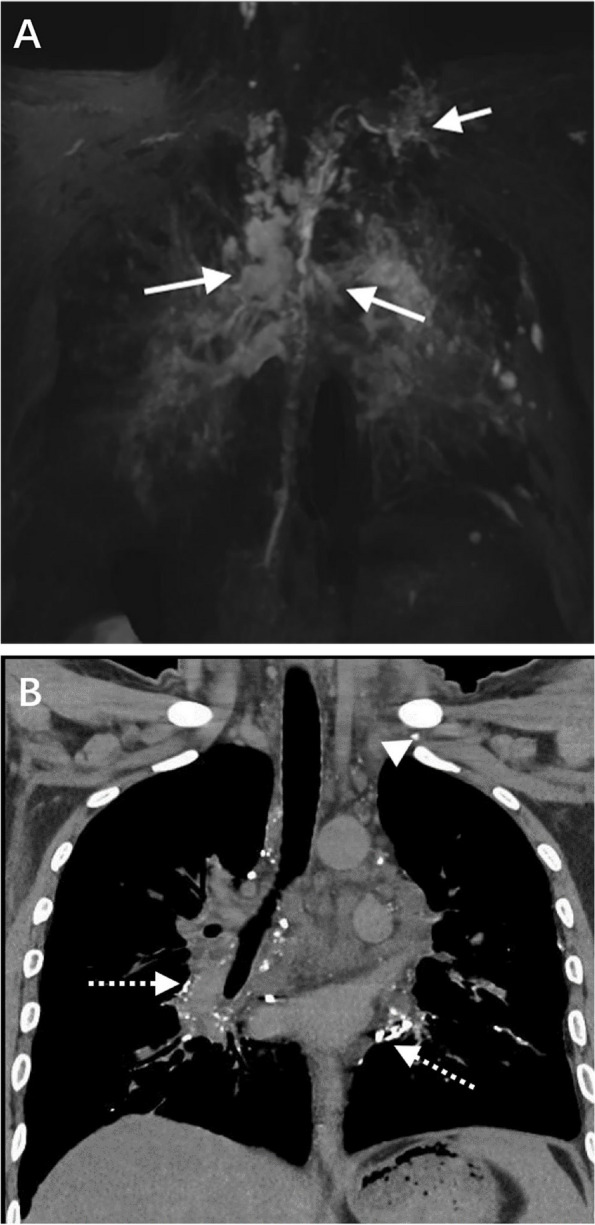
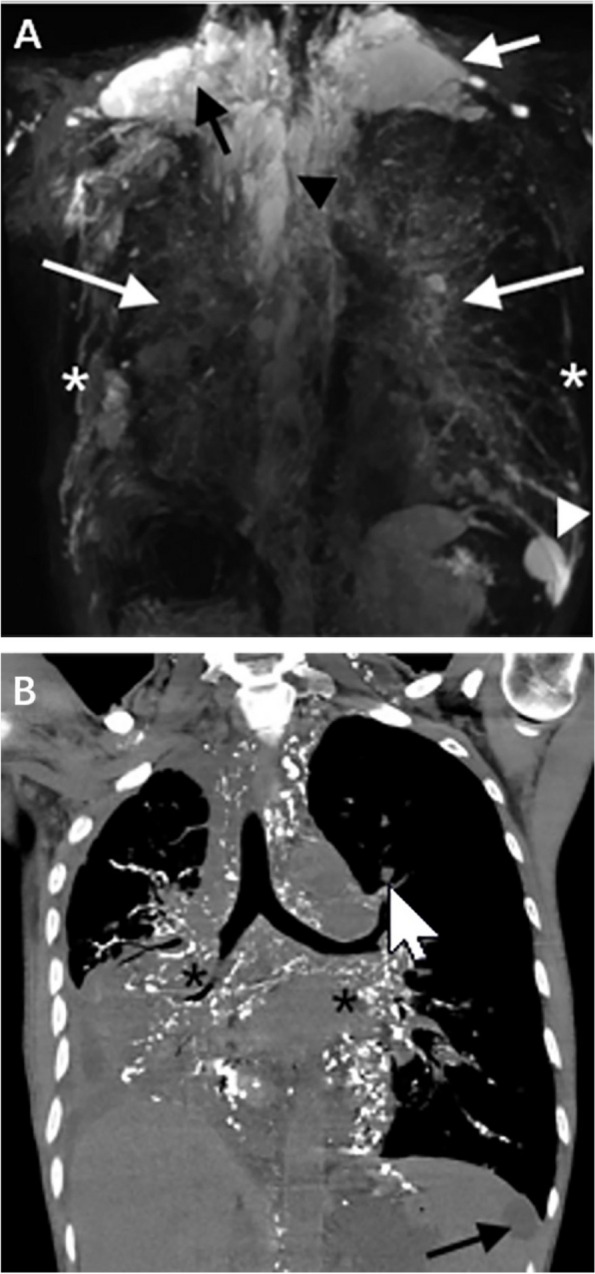
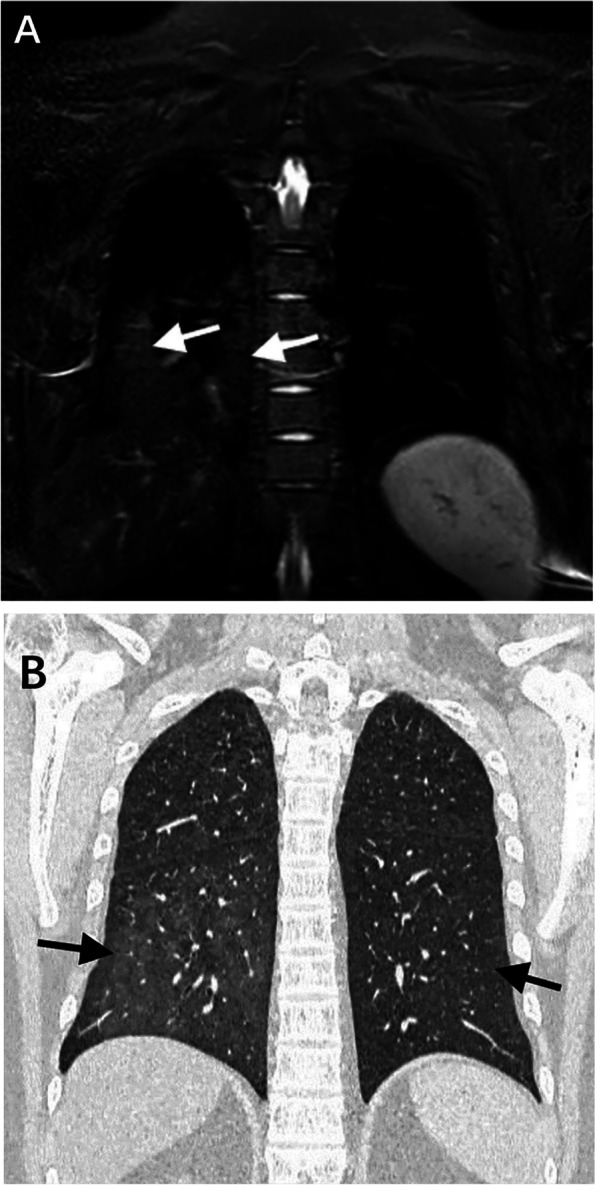
Materials and methods: The clinical and imaging data of 31 patients with lymphatic plastic bronchitis diagnosed by clinical, imaging and pathological results were retrospectively analyzed. All patients underwent CTL and MRL. The imaging findings of patients include: (i) abnormal lymphatic reflux of the bronchial mediastinal trunk, the subclavian trunk, the cervical trunk, the thoracic duct and the right lymphatic duct; Abnormal CTL reflux refers to abnormal iodide deposition outside the normal lymphatic reflux pathway; If the MRL can observe abnormal lymphatic dilatation, hyperplasia, or morphological abnormalities, it is assumed that abnormal lymphatic reflux may be present.; (ii) abnormal morphological changes of lymphatic vessels at the extremity of the thoracic duct, the extremity of the right lymphatic duct and the mediastinum, such as spot-like or tubular, cystic changes; (iii) abnormal CTL and MRL signs in the lungs. The Mcnemar test was used to compare the parameters between CTL and MRL. P< 0.05 was statistically significant. The Kappa test was used to evaluate the consistency of CTL and MRL in evaluating lymphatic plastic bronchitis.
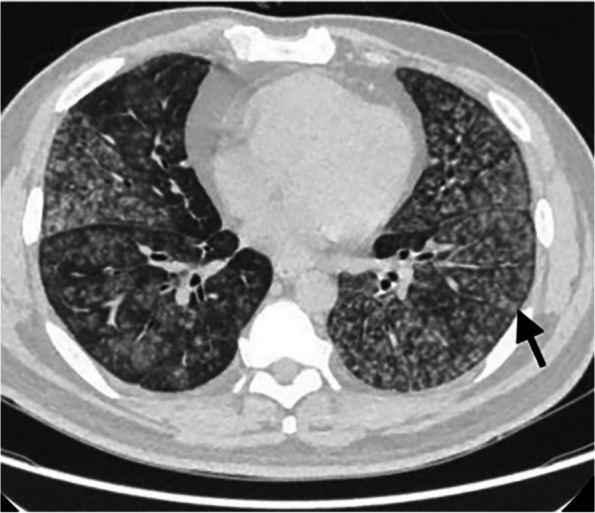
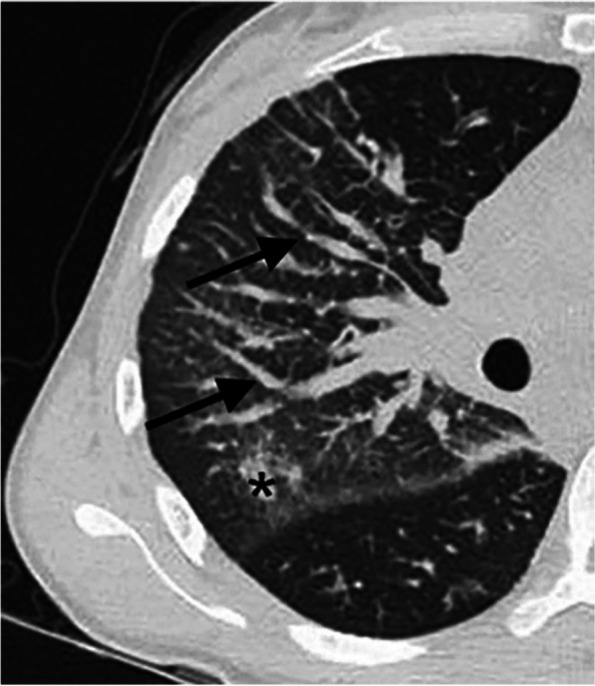
Results: MRL was superior to CTL in detecting abnormal lymphatic reflux in the right lymphatic vessel, thoracic duct, cervical trunk and subclavian trunk (P< 0.05).and the diagnostic consistency was general (Kappa < 0.40). There was no significant difference between MRL and CTL in the detection of abnormal lymphatic reflux in the bronchial mediastinal trunk (P> 0.05), and the diagnostic consistency was good (Kappa > 0.60). MRL was superior to CTL in detecting lymphatic abnormalities such as cystic changes at the extremity of the thoracic duct, spot-like or tubular changes at the extremity of the right lymphatic duct, cystic changes at the extremity of the right lymphatic duct, and cystic changes in the mediastinum (P< 0.05), and the diagnostic consistency was poor, fair, fair, and moderate (Kappa < 0.60), respectively. MRL and CTL showed abnormal signs in the lung: CTL was superior to MRL in showing the thickening of interlobular septum, lung nodules and airway stenosis (P< 0.05), and the diagnostic consistency was moderate, moderate and poor (Kappa < 0.60). There was no significant difference between CTL and MRL in atelectasis, consolidation in lobar and segmental distribution, consolidation in non-lobar and segmental distribution, and the thickening of the bronchovascular bundle (P> 0.05), and the diagnostic consistency was very good, very good, good, good (Kappa > 0.60). There was no significant difference between CTL and MRL in ground glass opacity, airway wall thickening and intralobular interstitial thickening (P> 0.05), and the diagnostic consistency was average, fair and poor (Kappa < 0.40).
Conclusion: The MRL is superior to CTL in showing the abnormalities of the thoracic duct, the right lymphatic duct and other abnormal lymphatic vessels. CTL is superior to MRL in the detection of pulmonary abnormalities. The combination of CTL and MRL can provide more comprehensive imaging information for diagnosing and treating lymphatic plastic bronchitis.
Keywords: Lymphangiography; Lymphatic; Magnetic resonance imaging; Plastic bronchitis; Tomography, X-ray.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Ethics Committee of Beijing Shijitan Hospital, Capital Medical University, and informed consent was waived because the study was retrospective review. Consent for publication: The images are entirely unidentifiable and there are no details on individuals reported within the manuscript. Competing interests: The authors declare no competing interests.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
