

Multimodality Imaging Supports Cardiac Lesion Diagnosis in Patient With Liver Carcinoma: A Case Report
- PMID: 39716413
- PMCID: PMC11666475
- DOI: 10.1002/cnr2.70088
Multimodality Imaging Supports Cardiac Lesion Diagnosis in Patient With Liver Carcinoma: A Case Report
Abstract
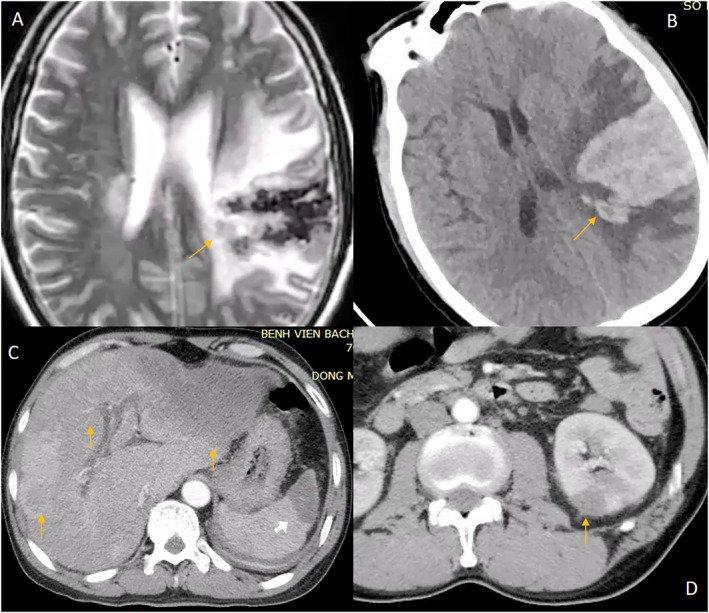
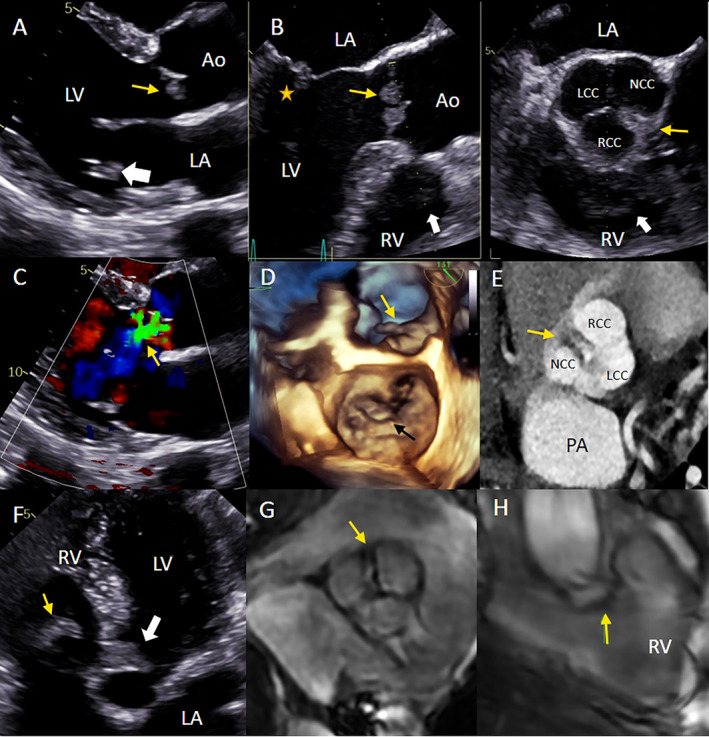
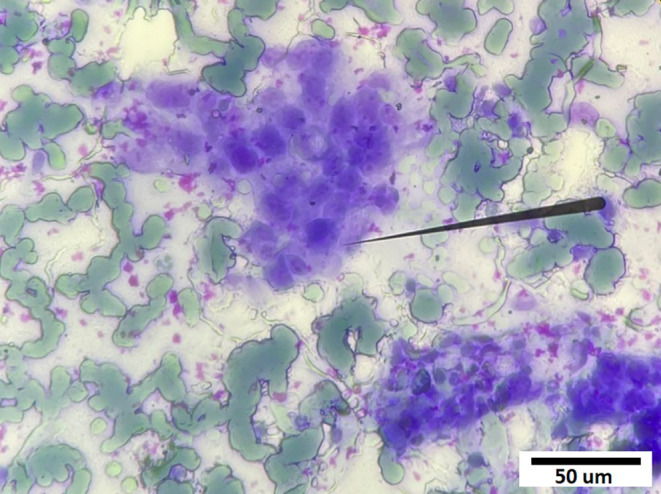
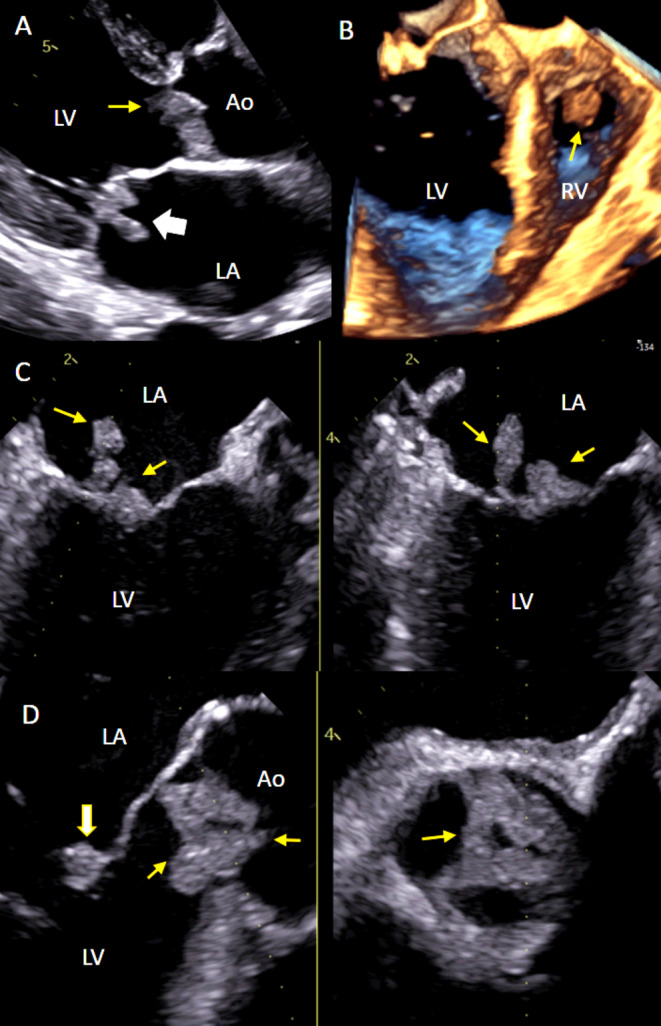
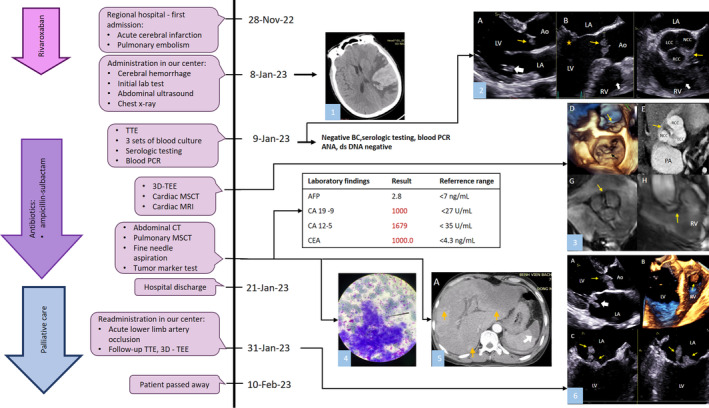
Introduction: Nonbacterial thrombotic endocarditis (NBTE) is a rare cardiac manifestation in patients with advanced malignancies of the lungs, pancreas, gynecological system, and gastrointestinal tract. It is often confirmed postmortem by histopathological evidence of sterile platelet-fibrin deposits attached to the endocardium, most often on heart valves. To the best of our knowledge, our case is the first to report multiple heart lesions caused by the systemic effect of cholangiocarcinoma.
Case presentation: We report the case of a 53-year-old male who presented with a stroke; extensive imaging studies, including transthoracic echocardiography (TTE), 2D/3D transesophageal echocardiography (TEE), cardiac multi-slice computed tomography, and cardiac magnetic resonance, found masses on the mitral valve, the aortic valve, and in the right ventricle, with the largest diameter 43 × 11 mm, which led to a diagnosis of NBTE secondary to presumed cholangiocarcinoma. Combining different echocardiography techniques, including TTE and TEE in specific clinical contexts, and training echocardiographers to improve TEE interpretation skills could be the most cost-effective option for early diagnosis, particularly in limited-resource settings, where advanced imaging modalities are not widely applicable.
Conclusions: NBTE can manifest in patients with advanced cancer. A high index of clinical suspicion is of central importance for the diagnosis of NBTE, especially through an identification of the underlying predisposing conditions. A multi-disciplinary approach is crucial for NBTE optimal diagnosis and treatment. As in our patient, multimodality imaging plays a complementary role in clearly defining the nature of cardiac lesions.
Keywords: cardiac magnetic resonance imaging; case report; liver adenocarcinoma; multimodality imaging; nonbacterial thrombotic endocarditis; three‐dimensional transesophageal echocardiography.
© 2024 The Author(s). Cancer Reports published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Nonbacterial Thrombotic Endocarditis Presenting with Leg Pain and a Left Atrial Mass Lesion.Cardiology. 2018;139(4):208-211. doi: 10.1159/000486635. Epub 2018 Feb 15. Cardiology. 2018. PMID: 29448257
-
Nonbacterial thrombotic endocarditis of a bioprosthetic valve: Questions to ponder before replacement of the valve.J Card Surg. 2020 May;35(5):1142-1144. doi: 10.1111/jocs.14536. Epub 2020 Apr 10. J Card Surg. 2020. PMID: 32275092
-
Fatal intracranial hemorrhage after intravenous thrombolytic therapy for acute ischemic stroke associated with cancer-related nonbacterial thrombotic endocarditis.J Stroke Cerebrovasc Dis. 2014 Sep;23(8):e413-e416. doi: 10.1016/j.jstrokecerebrovasdis.2014.04.004. Epub 2014 Aug 8. J Stroke Cerebrovasc Dis. 2014. PMID: 25126699
-
Non-bacterial thrombotic endocarditis: a rare presentation and literature review.BMJ Case Rep. 2020 Dec 13;13(12):e238585. doi: 10.1136/bcr-2020-238585. BMJ Case Rep. 2020. PMID: 33318278 Free PMC article. Review.
-
Nonbacterial Thrombotic Endocarditis: Pathogenesis, Diagnosis, and Management.Cardiol Rev. 2016 Sep-Oct;24(5):244-7. doi: 10.1097/CRD.0000000000000106. Cardiol Rev. 2016. PMID: 27501336 Review.
References
-
- Zadok O. I. B., Spectre G., and Leader A., “Cancer‐Associated Non‐Bacterial Thrombotic Endocarditis,” Thrombosis Research 213 (2022): S127–S132. - PubMed
-
- Brunton N., Kurmann R., Klarich K. W., Wysokinski W. E., Patrzalek P., and Casanegra A. I., “Non‐bacterial Thrombotic Endocarditis (NBTE) in the Absence of Malignancy or Autoimmune Disease: A Case Series,” Journal of the American College of Cardiology 83, no. 13_Supplement (2024): 2290.
-
- Steiner I., “Nonbacterial Thrombotic Endocarditis—A Study of 171 Case Reports,” Ceskoslovenská Patologie 29, no. 2 (1993): 58–60. - PubMed
-
- Patrzalek P., Wysokinski W. E., Kurmann R. D., et al., “Cancer‐Associated Non‐bacterial Thrombotic Endocarditis—Clinical Series From a Single Institution,” American Journal of Hematology 99, no. 4 (2024): 596–605. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
