

Optimal Antithrombotic Regimen After Cryptogenic Stroke: A Systematic Review and Network Meta-Analysis
- PMID: 39716815
- PMCID: PMC11672598
- DOI: 10.1177/10760296241309639
Optimal Antithrombotic Regimen After Cryptogenic Stroke: A Systematic Review and Network Meta-Analysis
Abstract
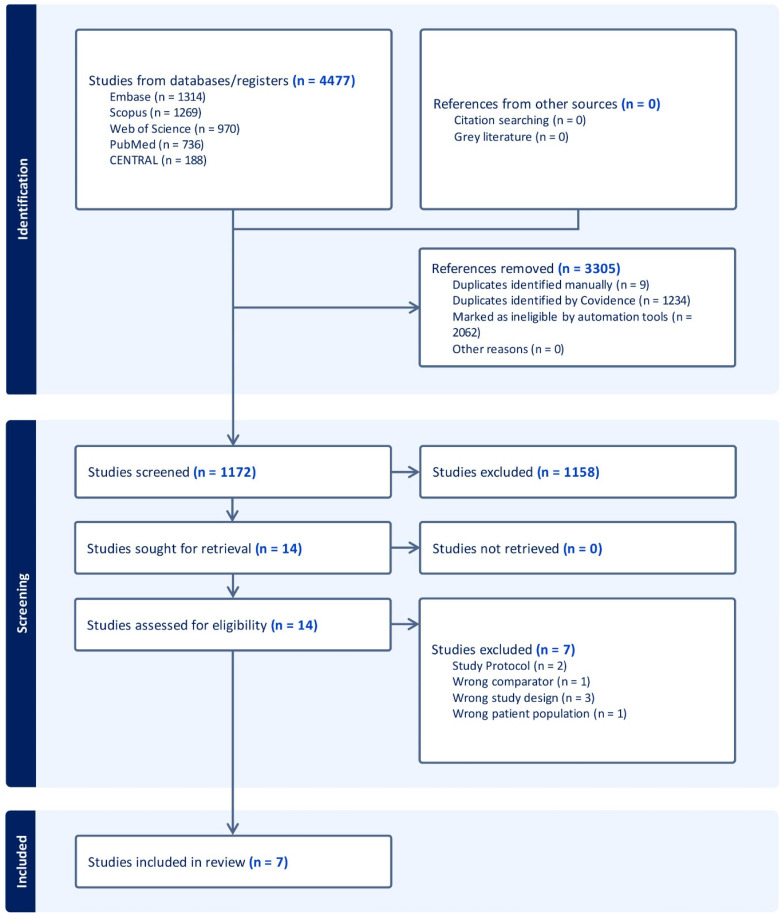
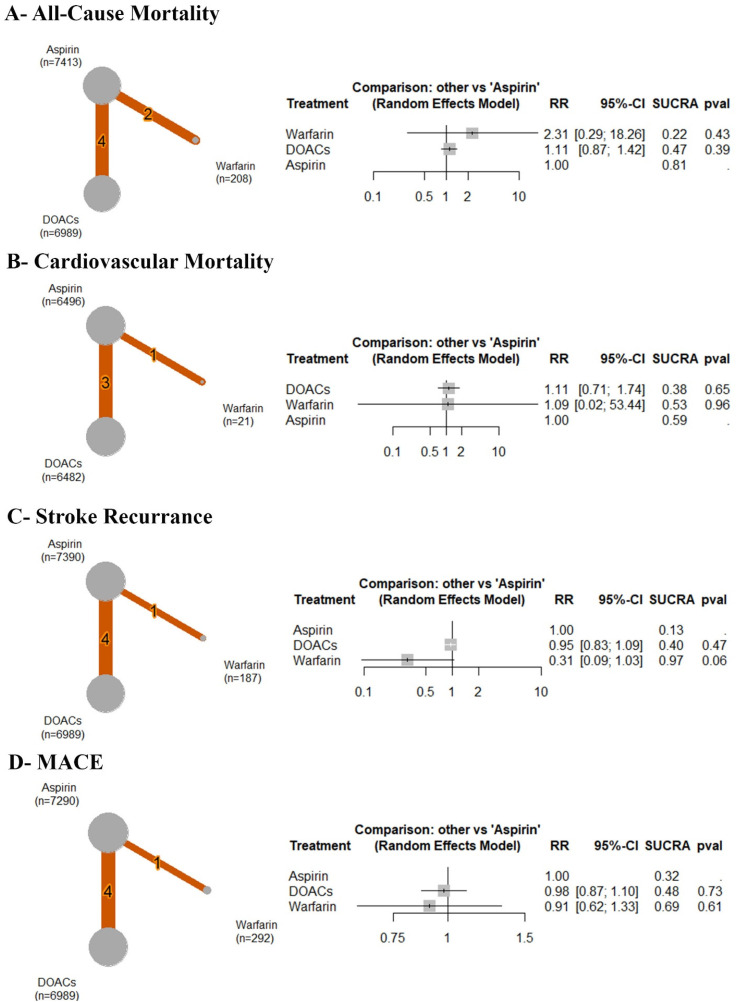
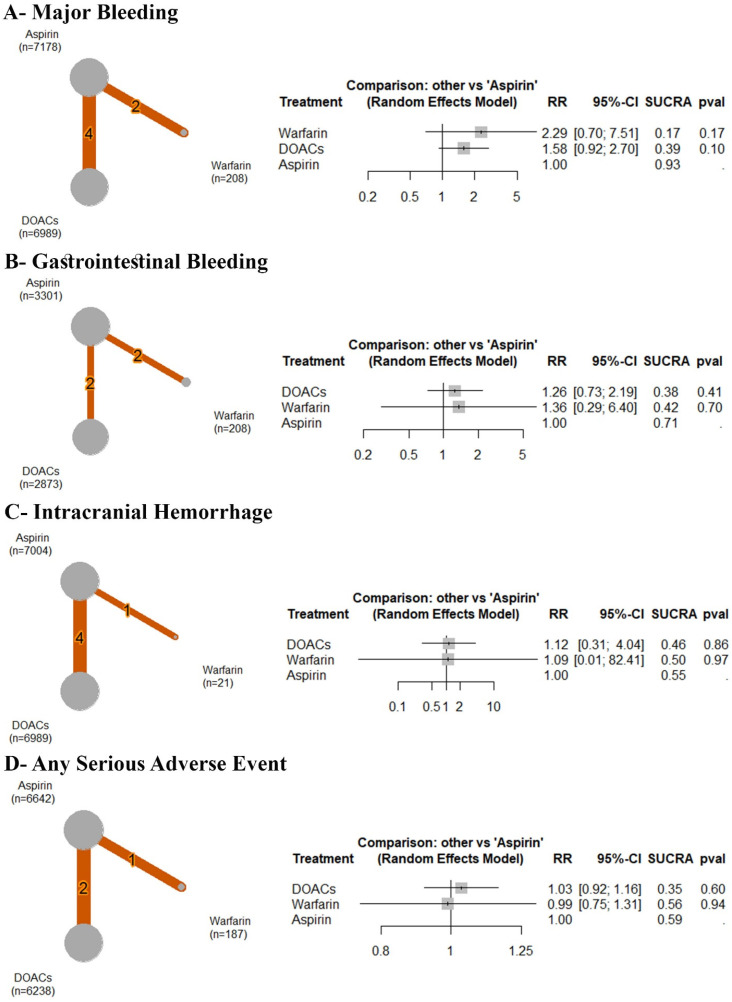
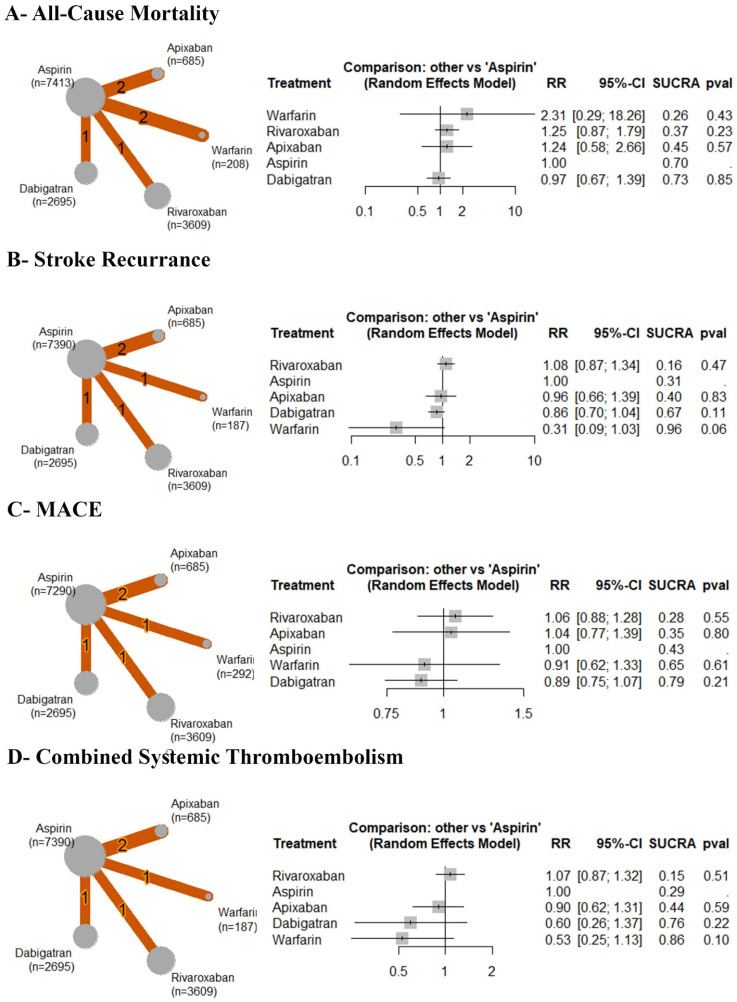
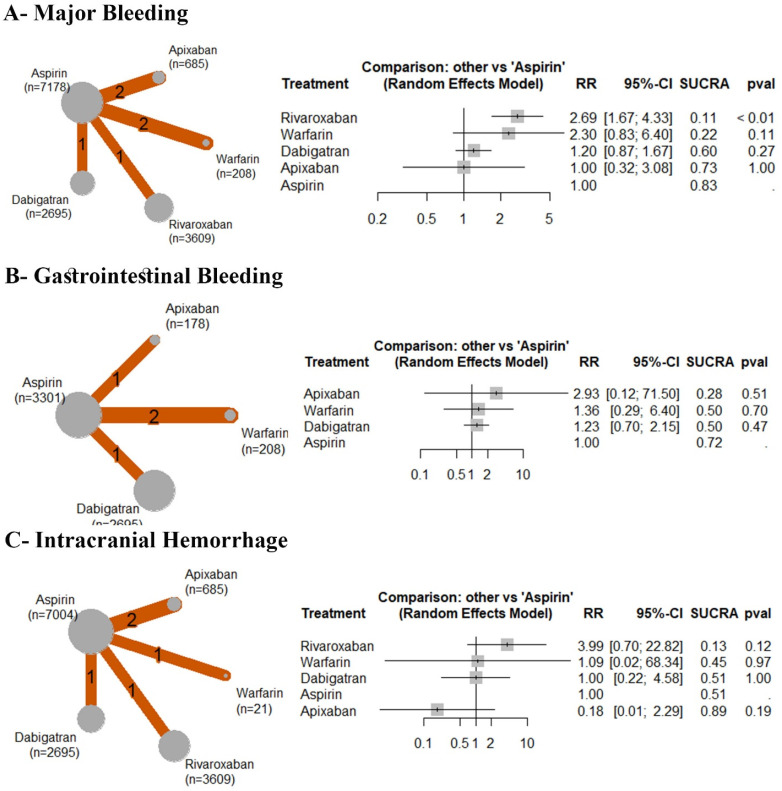
Although several antithrombotic strategies have been investigated for the management of cryptogenic strokes, ie, ischemic strokes without known etiologies, an optimal antithrombotic strategy for cryptogenic strokes is unknown. We aim to assess oral antithrombotic agents' comparative efficacy and safety after cryptogenic stroke to identify an optimal treatment.A systematic review and meta-analysis synthesizing evidence from randomized controlled trials (RCTs) obtained from PubMed, Embase Cochrane, Scopus, and Web of Science until February 2024. We used the random-effects model to report dichotomous outcomes using a risk ratio (RR) with a 95% confidence interval (CI). Frequentist network meta-analysis was conducted using R, version 4.3.1.Seven RCTs with 15,240 patients were included. None of the OACs showed a significant efficacy in preventing all-cause mortality, stroke recurrence, cardiovascular mortality, and major adverse cardiac events compared to aspirin. Also, safety measures were similar between different OACs and aspirin regarding safety measures, including major bleeding, intracranial hemorrhage, and gastrointestinal bleeding. However, only rivaroxaban significantly increased the incidence of major bleeding (RR: 2.69, CI [1.67, 4.33]).There was no difference between various OACs and aspirin regarding efficacy and safety outcomes. There is a greater risk of major bleeding with rivaroxaban. Further research is still warranted to define a personalized strategy for selecting antithrombotic strategies after cryptogenic stroke on a case-by-case basis.
Keywords: ESUS; apixaban; aspirin; brain infarct; dabigatran; idiopathic; rivaroxaban; warfarin.
Conflict of interest statement
Declaration of Conflicting InterestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- Laurent D, Small CN, Goutnik M, Hoh B. Ischemic stroke. In: Acute care neurosurg by case manag pearls pitfalls [internet]. 2022. [cited 2024 Apr 14]:159-172. https://www.ncbi.nlm.nih.gov/books/NBK499997/
-
- Shatri G, Senst B. Acute Stroke. In: StatPearls [Internet]. 2023. [cited 2024 Apr 14]. https://www.ncbi.nlm.nih.gov/books/NBK535369/
-
- Tiu C, Băjenaru O, Radu R, Terecoasa O. Etiologic classification of ischemic stroke: Where do we stand ? Clin Neurol Neurosurg [Internet]. 2017;159:93-106. https://pdf.sciencedirectassets.com/271158/1-s2.0-S0303846717X00073/1-s2... - PubMed
-
- Sacco RL, Ellenberg JH, Mohr JP, et al. Infarcts of undetermined cause: The NINCDS stroke data bank. Ann Neurol. 1989;25:382-390. - PubMed
-
- Donnan GA. Cryptogenic stroke. Int J Stroke. 2017;12:919. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
