

Stereotactic cardiac radiotherapy for refractory ventricular tachycardia in structural heart disease patients: a systematic review
- PMID: 39716963
- PMCID: PMC11780863
- DOI: 10.1093/europace/euae305
Stereotactic cardiac radiotherapy for refractory ventricular tachycardia in structural heart disease patients: a systematic review
Abstract
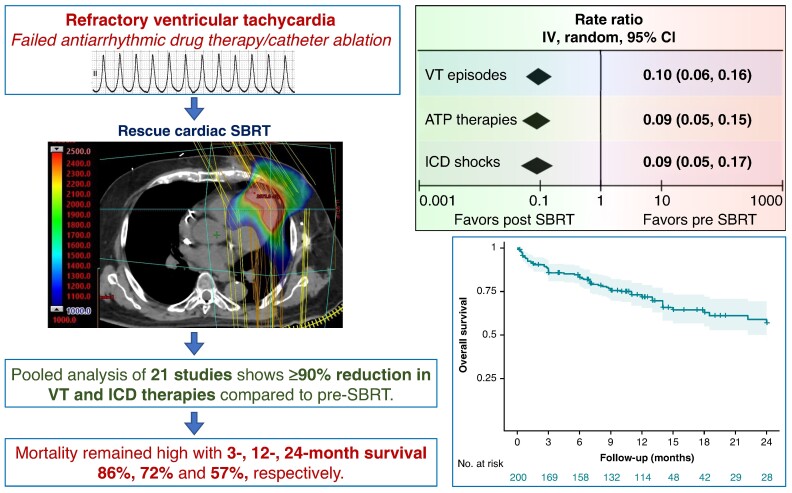
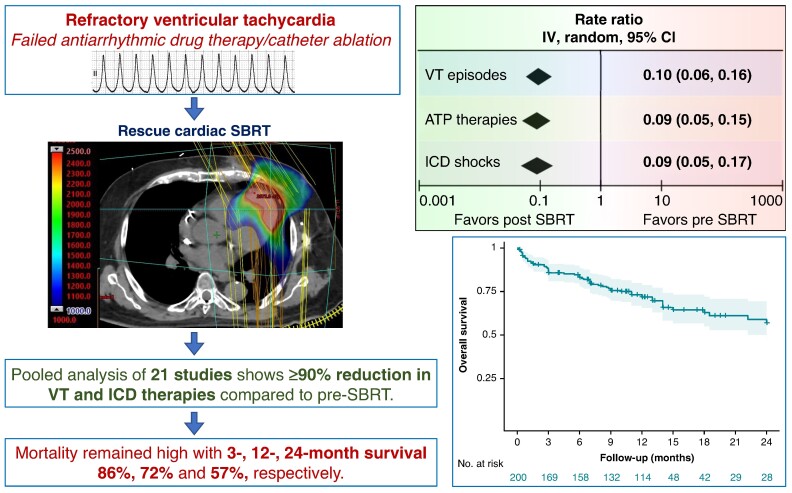
Aims: Among patients with structural heart disease with ventricular tachycardia (VT) refractory to medical therapy and catheter ablation, cardiac stereotactic body radiotherapy (SBRT) is a paradigm-changing treatment option. This study aims to assess the efficacy of cardiac SBRT in refractory VT by comparing the rates of VT episodes, anti-tachycardia pacing (ATP) therapies, and implantable cardioverter-defibrillator (ICD) shocks post-SBRT with pre-SBRT.
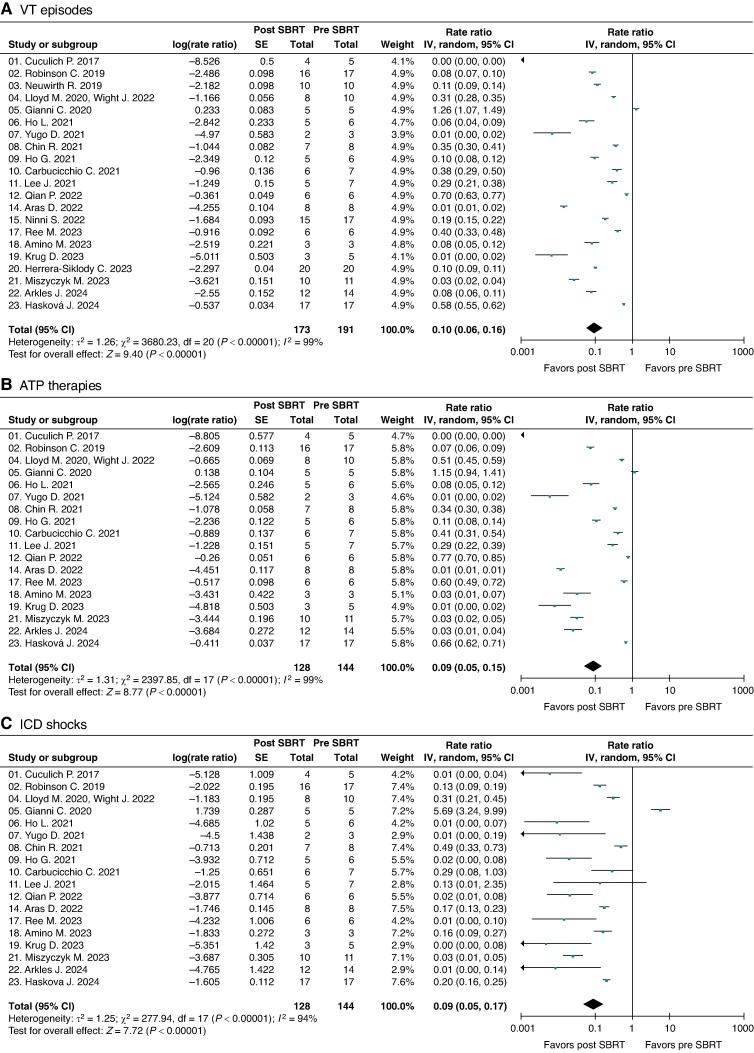
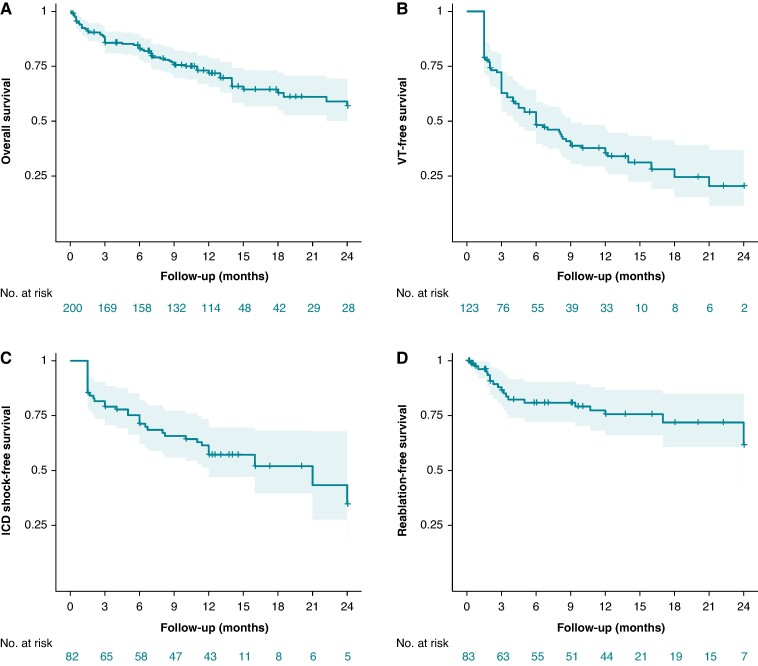
Methods and results: We performed a comprehensive literature search and included all clinical studies reporting outcomes on cardiac SBRT for VT. Treatment efficacy was evaluated as random-effects pooled rate-ratios of VT episodes, ATP therapies and ICD shocks post-SBRT (after 6-week blanking) and pre-SBRT, with patients serving as their own controls. Post-SBRT overall survival was assessed using Kaplan-Meier method. We included 23 studies published 2017-24 reporting on 225 patients who received cardiac SBRT, with median follow-up 5.8-28 months. There was significant heterogeneity among the studies for all three efficacy endpoints (P < 0.00001). The random-effects pooled rate-ratios of VT episodes, ATP therapies and ICD shocks post- vs. pre-SBRT were 0.10 (95% CI 0.06, 0.16), 0.09 (0.05, 0.15), and 0.09 (0.05, 0.17), respectively (all P < 0.00001). The most common reported complications included pericardial (8.0%, including 0.9% late oesophagogastro-pericardial fistula) and pulmonary (5.8%). There was no change in left ventricular ejection fraction post-SBRT (P = 0.3) but some studies reported an increase in mitral regurgitation. The combined 3-, 12-, and 24-month overall patient survival was 0.86 (0.80, 0.90), 0.72 (0.65, 0.78), and 0.57 (0.47, 0.67), respectively.
Conclusion: Among patients with refractory VT in context of structural heart disease, VT burden and ICD shocks are dramatically reduced following cardiac SBRT. The overall mortality in this population with heart failure and refractory VT receiving palliative cardiac SBRT remains high.
Keywords: Cardiac; Meta-analysis; Radioablation; Radiotherapy; SABR; SBRT; STAR; Stereotactic ablative body radiotherapy; Stereotactic arrhythmia radioablation; Stereotactic body radiotherapy; VT; Ventricular tachycardia.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: The authors have no relevant conflicts of interest to disclose.
Figures
Comment in
-
Aiming for the STARs: radiotherapy for ventricular tachycardia-bright future or cosmic gamble?Europace. 2024 Dec 26;27(1):euae306. doi: 10.1093/europace/euae306. Europace. 2024. PMID: 39716957 Free PMC article.
References
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med 2005;352:225–37. - PubMed
-
- Moss AJ, Schuger C, Beck CA, Brown MW, Cannom DS, Daubert JP et al. Reduction in inappropriate therapy and mortality through ICD programming. N Engl J Med 2012;367:2275–83. - PubMed
-
- Connolly SJ, Dorian P, Roberts RS, Gent M, Bailin S, Fain ES et al. Comparison of beta-blockers, amiodarone plus beta-blockers, or sotalol for prevention of shocks from implantable cardioverter defibrillators: the OPTIC study: a randomized trial. JAMA 2006;295:165–71. - PubMed
-
- Tung R, Vaseghi M, Frankel DS, Vergara P, Di Biase L, Nagashima K et al. Freedom from recurrent ventricular tachycardia after catheter ablation is associated with improved survival in patients with structural heart disease: an International VT Ablation Center Collaborative Group study. Heart Rhythm 2015;12:1997–2007. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
