

The waist-to-height ratio is a good predictor for insulin resistance in women with polycystic ovary syndrome
- PMID: 39717101
- PMCID: PMC11664359
- DOI: 10.3389/fendo.2024.1502321
The waist-to-height ratio is a good predictor for insulin resistance in women with polycystic ovary syndrome
Abstract
Objective: This study aimed to explore the role of the waist-to-height ratio (WHtR) in assessing insulin resistance (IR) in patients with polycystic ovary syndrome (PCOS).
Materials and methods: We enrolled 882 PCOS-afflicted women in a cross-sectional analysis to evaluate the association of the WHtR with IR. Their demographic characteristics, anthropometric parameters, and fasting blood samples were collected and measured. Moreover, IR was evaluated by homeostatic model assessment of insulin resistance (HOMA-IR). We estimated the relationship between the WHtR and IR and the cut-off thresholds of the WHtR for IR using multivariable linear regression and logistic regression models, respectively.
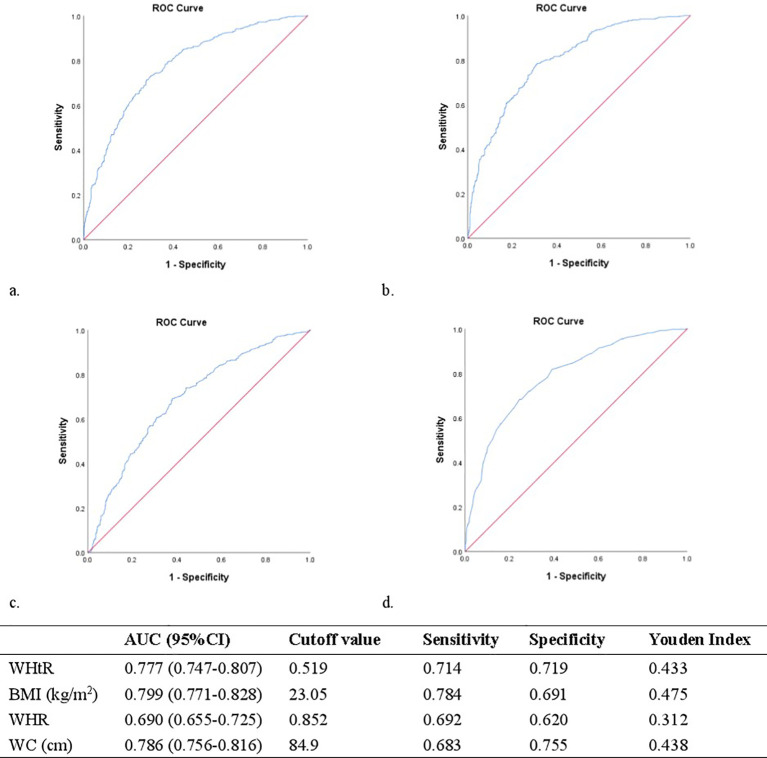
Results: The prevalence rate of IR was 51.9%. The patients with PCOS and IR displayed significantly increased values for body mass index (BMI), waist circumference (WC), WHtR, systolic blood pressure (SBP), diastolic blood pressure (DBP), free androgen index (FAI), HOMA-IR, total cholesterol (TC), triglyceride (TG), low-density lipoprotein cholesterol (LDL-C), and apolipoprotein B (ApoB). However, the patients with PCOS and IR showed a reduction in estradiol (E2), luteinizing hormone (LH), LH/FSH ratio, sex hormone binding globulin (SHBG), and high-density lipoprotein (HDL-C) values than those without IR. Moreover, BMI (log-transformed), WC, and HOMA-IR (log-transformed) were positively correlated with the WHtR. When adjusting for potential confounding variables, the WHtR was significantly associated with HOMA-IR (log-transformed), with a standardized regression coefficient of 0.271. Furthermore, the WHtR was significantly associated with an increased risk of IR, with the adjusted odds ratio (OR) of 3.15 (WHtR multiplied by 10). Additionally, the WHtR helped to identify IR in women with PCOS with an optimal cut-off point of 0.519 (Youden index = 0.433).
Conclusions: The WHtR had a positive association with IR in women with PCOS. Hence, we suggest that the WHtR, as a simple, practical, and reliable anthropometric measure, can be used to predict the risk of IR in patients with PCOS.
Keywords: anthropometric measurements; insulin resistance; polycystic ovary syndrome; prediction; waist-to-height ratio.
Copyright © 2024 Zhu, Wang, Feng, Liu, Guan, Wang and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous