

Efficacy and safety of misoprostol compared with dinoprostone for labor induction at term: an updated systematic review and meta-analysis of randomized controlled trials
- PMID: 39717175
- PMCID: PMC11664862
- DOI: 10.3389/fmed.2024.1459793
Efficacy and safety of misoprostol compared with dinoprostone for labor induction at term: an updated systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Labor induction is a common obstetric intervention, increasingly performed worldwide, often using prostaglandins like misoprostol and dinoprostone.
Objective: This study aims to compare the effectiveness and safety of intravaginal misoprostol versus dinoprostone for inducing labor, examining their impact on various maternal and neonatal outcomes.
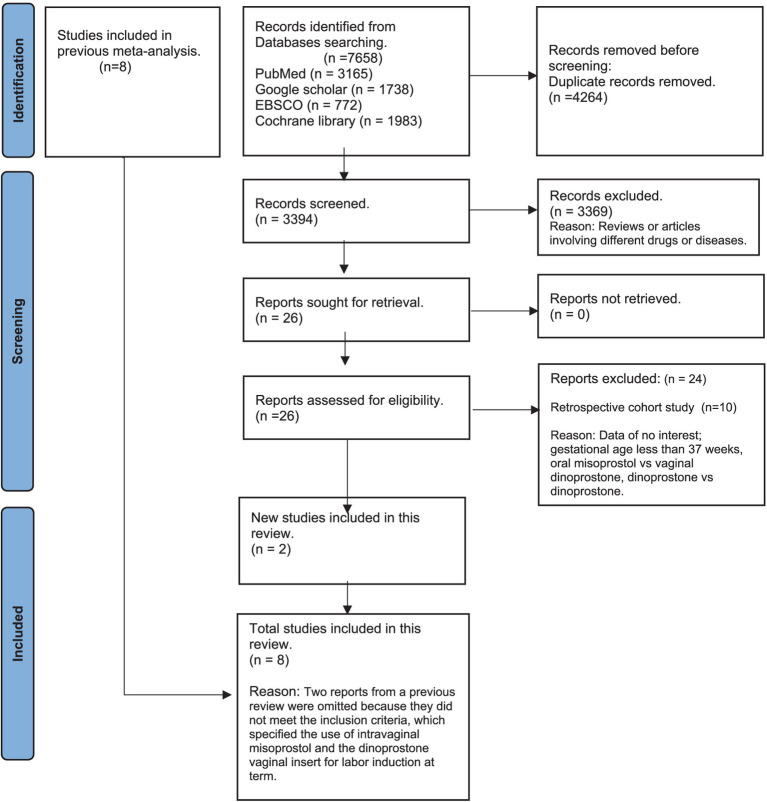
Methods: A systematic review and meta-analysis were conducted using four databases-PubMed, Google Scholar, EBSCO, and the Cochrane Library-from January 2000 to April 2023. We included randomized controlled trials (RCTs) involving singleton pregnancies at term (37-42 weeks) with unfavorable cervices, where intravaginal misoprostol was compared to dinoprostone. Key outcomes evaluated for effectiveness included vaginal delivery within 24 h, overall vaginal delivery rate, and need for oxytocin augmentation. Safety outcomes assessed were tachysystole, uterine hyperstimulation, abnormal cardiotocography, NICU admissions, cesarean delivery, and APGAR scores. Risk ratios (RRs) and 95% confidence intervals (CIs) were calculated using a random-effects model in Review Manager (RevMan) version 5.4.1.
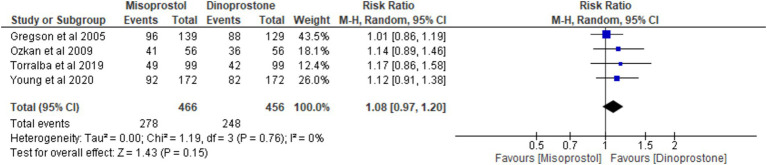
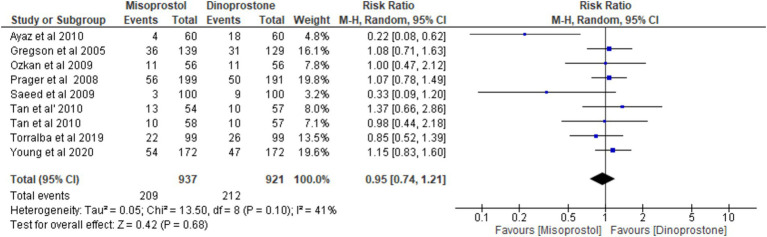
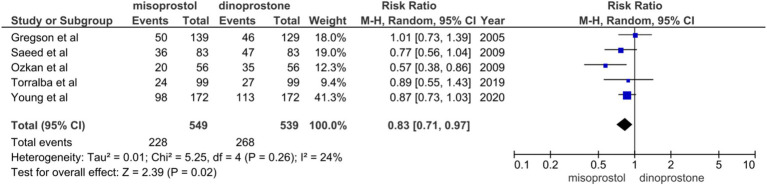
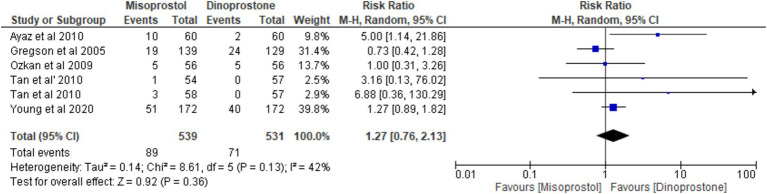
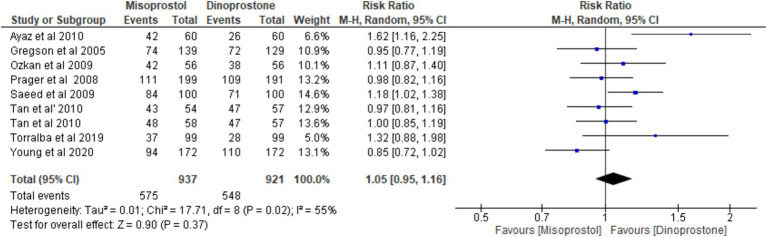
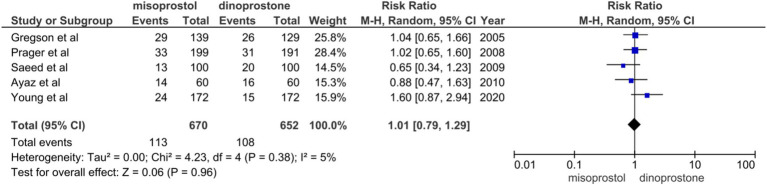
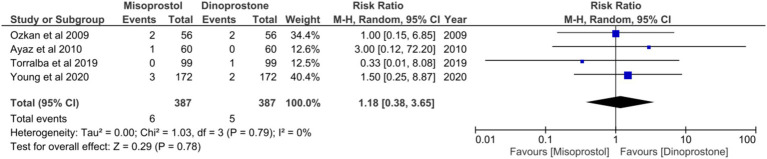
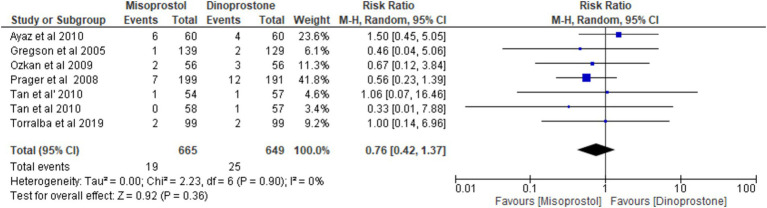
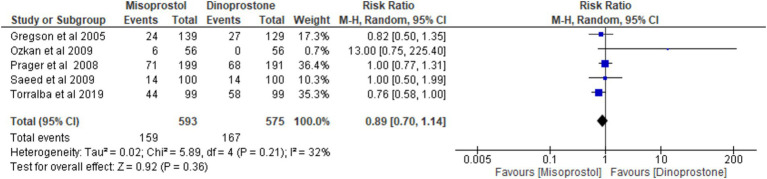
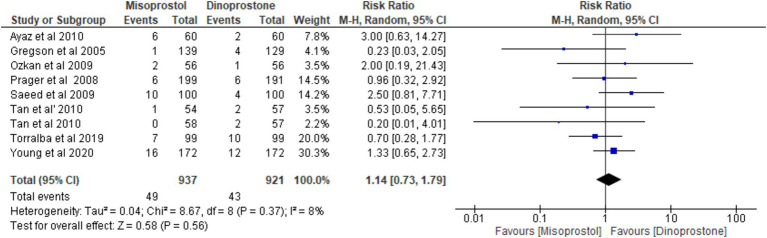
Results: Eight RCTs with a total of 1,801 participants (937 in the misoprostol group and 864 in the dinoprostone group) met the inclusion criteria. Misoprostol required a significantly less oxytocin augmentation than dinoprostone [RR = 0.83; 95% CI (0.71, 0.97), p = 0.02]. Other outcomes, including rates of cesarean delivery, uterine tachysystole, hyperstimulation, and NICU admissions, showed no significant differences between the two groups, indicating comparable safety and efficacy profiles.
Conclusion: This meta-analysis demonstrates that intravaginal misoprostol is an effective and safe alternative to dinoprostone for labor induction at term. Misoprostol achieved comparable efficacy and safety outcomes while requiring less oxytocin augmentation, supporting its potential as a practical induction agent in clinical settings.
Keywords: dinoprostone; intravaginally; labor induction; misoprostol; term.
Copyright © 2024 Lakho, Hyder, Ashraf, Khan, Kumar, Jabbar, Kumari, Qammar, Kumar, Kumari, Deepak, Raj and Ali.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Martin JA, Hamilton BE, Ventura SJ, Osterman MJ, Kirmeyer S, Mathews TJ, et al. Births: final data for 2009. Natl Vital Stat Rep. 60:1–70. PMID: - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous