

Laparoscopic vs. open portoenterostomy for biliary atresia: a meta-analysis of pediatric surgical outcomes
- PMID: 39717191
- PMCID: PMC11663641
- DOI: 10.3389/fped.2024.1476195
Laparoscopic vs. open portoenterostomy for biliary atresia: a meta-analysis of pediatric surgical outcomes
Abstract
Background: The pivotal importance of surgical treatment for pediatric biliary atresia is well-established. This systematic review and meta-analysis was designed to assess the comparative efficacy and safety of open portoenterostomy (OPE) and laparoscopic portoenterostomy (LPE) in managing this condition, providing valuable guidance for clinical decision-making.
Methods: A comprehensive literature review was conducted by two researchers in databases such as PubMed, up to July 10, 2024, focusing on studies that evaluated the role of LPE vs. OPE. Data analysis was performed utilizing the RevMan 5.4 software suite.
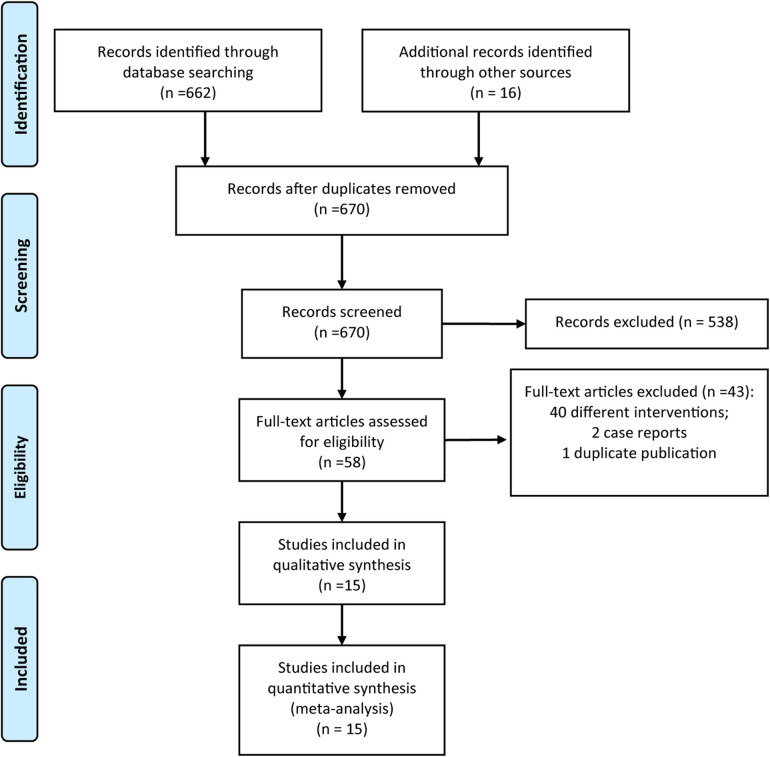
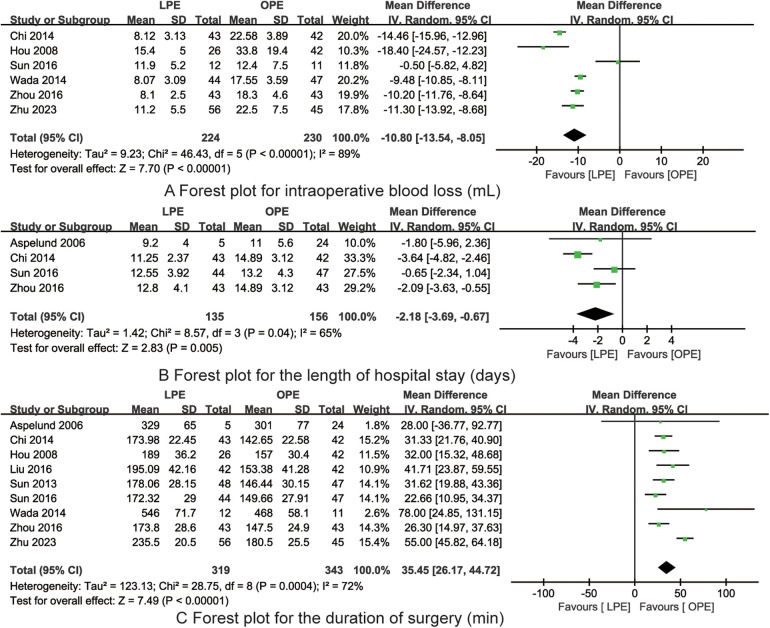
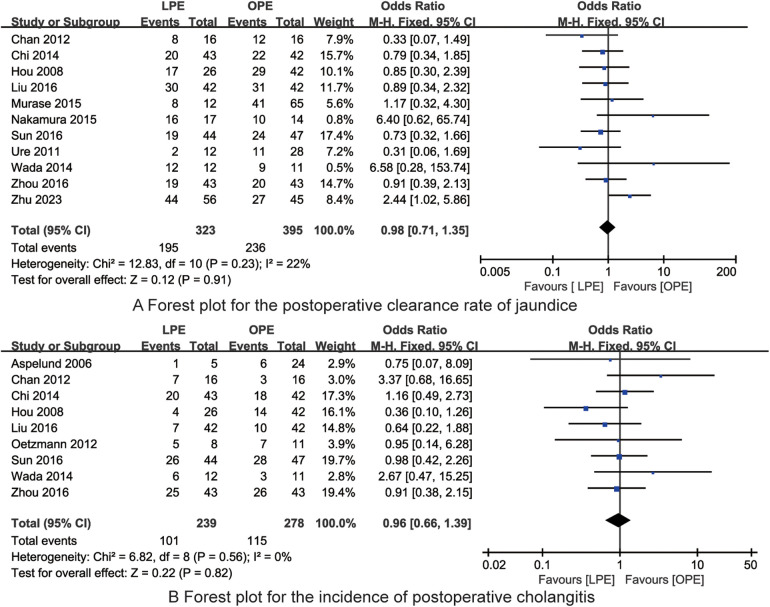
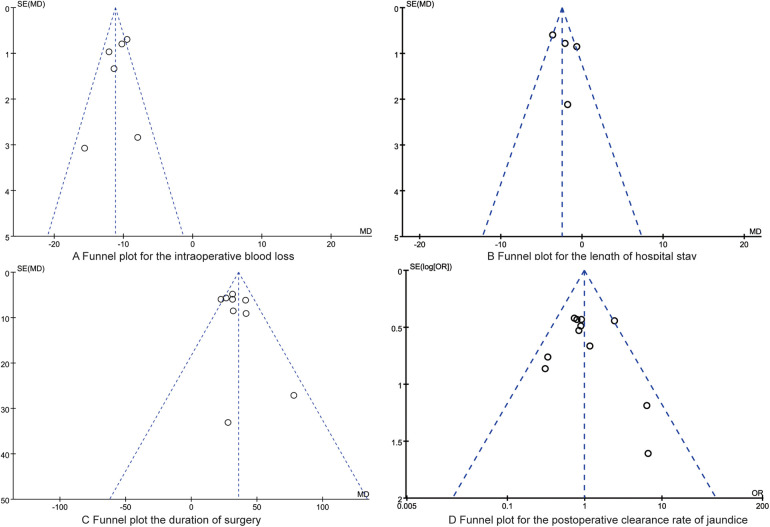
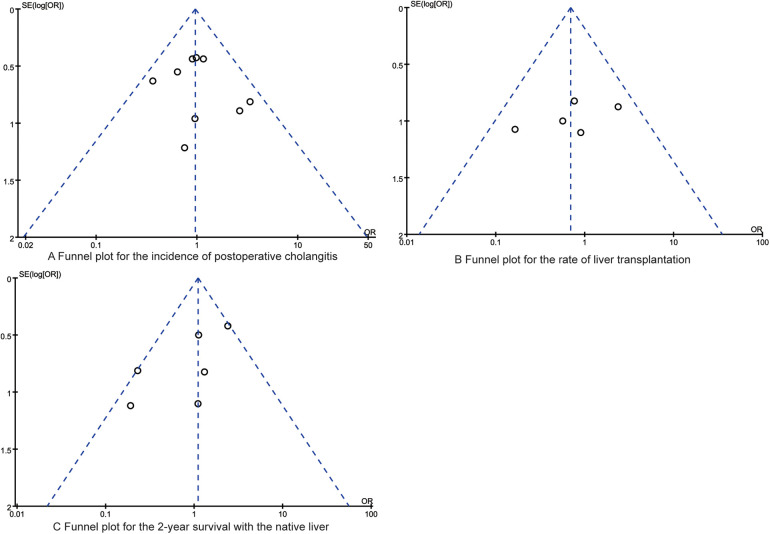
Results: The meta-analysis incorporated findings from 15 studies involving a total of 964 pediatric patients with biliary atresia. LPE was associated with decreased intraoperative blood loss [Mean Difference (MD) = -10.80, 95% Confidence Interval (CI) (-13.54, -8.05)] and shortened hospital stay [MD = -2.18, 95% CI (-3.69, -0.67)]. Conversely, the operative time for LPE was considerably longer when compared to OPE [MD = 35.45, 95% CI (26.17, 44.72)]. No significant disparities were noted in the postoperative jaundice clearance rate [Odds Ratio (OR) = 0.98, 95% CI (0.71, 1.35)], incidence of postoperative cholangitis [OR = 0.96, 95% CI (0.66, 1.39)], the rate of liver transplantation between the two surgical approaches [OR = 0.69, 95% CI (0.32, 1.48)], or 2-year survival of the native liver [OR = 1.10, 95% CI (0.67, 1.80)].
Conclusion: LPE offers more advantages over OPE, including diminished invasiveness and expedited recovery. These benefits suggest that LPE is an emerging and viable alternative in the clinical management of biliary atresia, warranting further investigation and consideration in surgical practice.
Keywords: biliary atresia; children; laparoscopy; portoenterostomy; surgery; treatment.
© 2024 Zhu, Wu, Cai, Pan and Zhu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Comparison of laparoscopic portoenterostomy and open portoenterostomy for the treatment of biliary atresia.Surg Endosc. 2019 Oct;33(10):3143-3152. doi: 10.1007/s00464-019-06905-9. Epub 2019 Jun 12. Surg Endosc. 2019. PMID: 31190228
-
Laparoscopic versus open portoenterostomy for treatment of biliary atresia: a meta-analysis.Pediatr Surg Int. 2023 Mar 7;39(1):148. doi: 10.1007/s00383-023-05436-8. Pediatr Surg Int. 2023. PMID: 36881201
-
Laparoscopic portoenterostomy versus open portoenterostomy for the treatment of biliary atresia: a systematic review and meta-analysis of comparative studies.Pediatr Surg Int. 2015 Mar;31(3):261-9. doi: 10.1007/s00383-015-3662-7. Epub 2015 Jan 28. Pediatr Surg Int. 2015. PMID: 25627699
-
Comprehensive assessment of prognosis after laparoscopic portoenterostomy for biliary atresia.Pediatr Surg Int. 2016 Feb;32(2):109-12. doi: 10.1007/s00383-015-3820-y. Epub 2015 Oct 31. Pediatr Surg Int. 2016. PMID: 26520656
-
Biochemical Evaluation of Laparoscopic Portoenterostomy for Treating Biliary Atresia and Redo for Failed Portoenterostomy.J Laparoendosc Adv Surg Tech A. 2022 Dec;32(12):1212-1219. doi: 10.1089/lap.2022.0245. Epub 2022 Aug 8. J Laparoendosc Adv Surg Tech A. 2022. PMID: 35939285
References
Publication types
LinkOut - more resources
Full Text Sources