

Intrathecal Morphine and Ropivacaine for Quality of Recovery After Laparoscopic Colorectal Surgery: A Randomized Controlled Trial
- PMID: 39717198
- PMCID: PMC11664109
- DOI: 10.2147/DDDT.S500316
Intrathecal Morphine and Ropivacaine for Quality of Recovery After Laparoscopic Colorectal Surgery: A Randomized Controlled Trial
Abstract
Purpose: Intrathecal morphine is increasingly used for pain management in laparoscopic colorectal surgery. While ropivacaine shows advantages of reduced cardiotoxicity and faster motor recovery compared to bupivacaine, the impact of intrathecal morphine-ropivacaine combination on postoperative recovery quality remains unclear. This study aimed to evaluate this combination's effect on recovery outcomes after laparoscopic colorectal surgery.
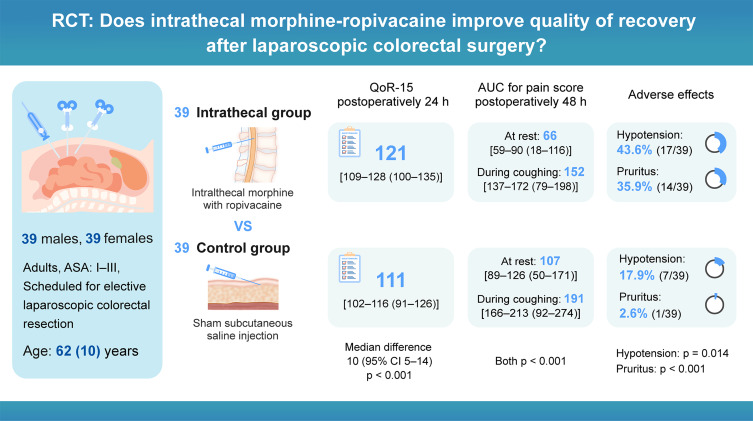
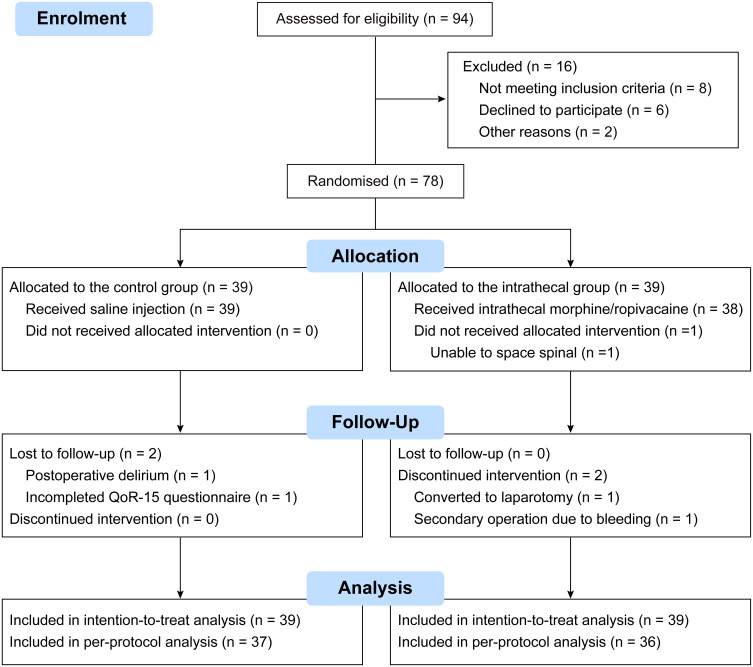
Patients and methods: In this randomized, double-blind, placebo-controlled trial, 78 patients undergoing laparoscopic colorectal surgery received either preservative-free intrathecal morphine 250 μg with ropivacaine 15 mg (Intrathecal group) or a sham subcutaneous saline injection (Control group). The primary outcome was the Quality of Recovery-15 (QoR-15) score 24 hours after surgery. Secondary outcomes included pain scores, opioid consumption, and adverse effects.
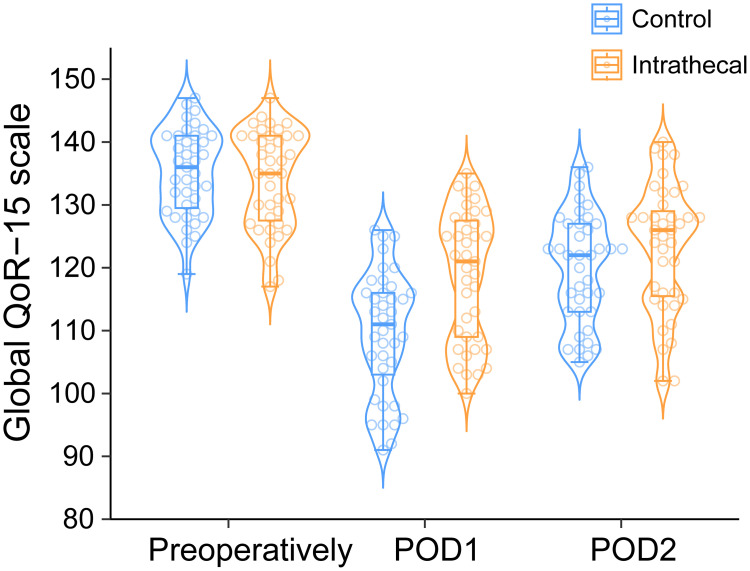
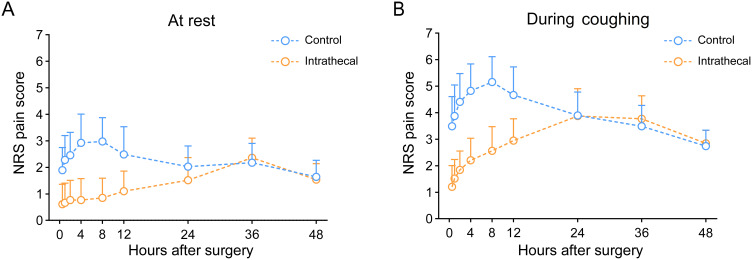
Results: The intrathecal group showed significantly higher QoR-15 scores 24 hours postoperatively compared to the control group (median [IQR]: 121 [109-128] vs 111 [102-116], p < 0.001), with improvements in pain management (p < 0.001), physical comfort (p = 0.001), and physical independence (p = 0.002). The intrathecal group had lower pain scores at rest (area under the curve 0-48 h: 66 [59-90] vs 107 [89-126], p < 0.001) and during coughing (152 [137-172] vs 191 [166-213], p < 0.001), particularly from 0.5 to 24 hours. They also required less postoperative morphine (0-48 h: 10 [6-20] vs 26 [22-36] mg, p < 0.001). While hypotension (43.6% vs 17.9%, p = 0.014) and pruritus (35.9% vs 2.6%, p < 0.001) were more frequent in the intrathecal group, but no respiratory depression occurred in either group.
Conclusion: Intrathecal morphine-ropivacaine administration improves 24-hour postoperative recovery quality and provides superior pain relief after laparoscopic colorectal surgery, despite increased but manageable side effects. Further research should focus on dose optimization and comparative studies of different intrathecal local anesthetic combinations.
Trial registration: The Chinese Clinical Trial Registry, ChiCTR2100052337.
Keywords: intrathecal morphine; laparoscopic colorectal surgery; pain management; quality of recovery; ropivacaine.
© 2024 Yang et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
No Difference in Early Analgesia Between Liposomal Bupivacaine Injection and Intrathecal Morphine After TKA.Clin Orthop Relat Res. 2017 Jan;475(1):94-105. doi: 10.1007/s11999-016-4931-z. Clin Orthop Relat Res. 2017. PMID: 27339124 Free PMC article. Clinical Trial.
-
Transmuscular quadratus lumborum (TQL) block for laparoscopic colorectal surgery: study protocol for a double-blind, prospective randomized placebo-controlled trial.Trials. 2020 Jun 26;21(1):581. doi: 10.1186/s13063-020-04525-6. Trials. 2020. PMID: 32586361 Free PMC article.
-
Intrathecal Morphine for Laparoscopic Segmental Colonic Resection as Part of an Enhanced Recovery Protocol: A Randomized Controlled Trial.Reg Anesth Pain Med. 2018 Feb;43(2):166-173. doi: 10.1097/AAP.0000000000000703. Reg Anesth Pain Med. 2018. PMID: 29219935 Free PMC article. Clinical Trial.
-
Analgesic efficacy of intrathecal morphine and bupivacaine during the early postoperative period in patients who underwent robotic-assisted laparoscopic prostatectomy: a prospective randomized controlled study.BMC Urol. 2021 Feb 26;21(1):30. doi: 10.1186/s12894-021-00798-4. BMC Urol. 2021. PMID: 33637066 Free PMC article. Clinical Trial.
-
The use of intrathecal morphine in non-abdominal surgery: a scoping review.BJA Open. 2025 Mar 20;14:100387. doi: 10.1016/j.bjao.2025.100387. eCollection 2025 Jun. BJA Open. 2025. PMID: 40223919 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
