

Physiological versus time based cord clamping in very preterm infants (ABC3): a parallel-group, multicentre, randomised, controlled superiority trial
- PMID: 39717227
- PMCID: PMC11664066
- DOI: 10.1016/j.lanepe.2024.101146
Physiological versus time based cord clamping in very preterm infants (ABC3): a parallel-group, multicentre, randomised, controlled superiority trial
Abstract
Background: Physiological-based cord clamping (PBCC) in preterm infants is beneficial for cardiovascular transition at birth and may optimize placental transfusion. Whether PBCC can improve clinical outcomes is unknown. The aim of the Aeration, Breathing, Clamping (ABC3) trial was to test whether PBCC results in improved intact survival in very preterm infants.
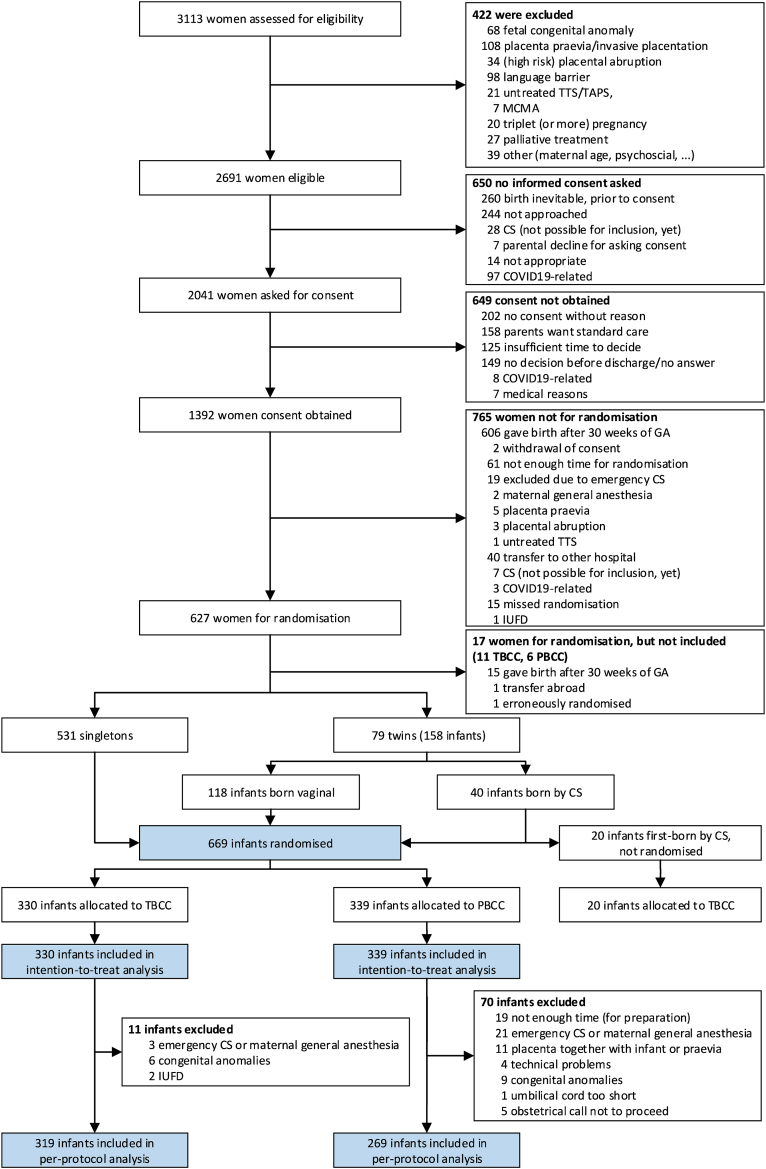
Methods: The ABC3 trial was a parallel-group, multicentre, randomised, controlled superiority clinical trial conducted in all Dutch tertiary referral centers for perinatal care involving infants born before 30 weeks of gestation. Infants were randomised to either PBCC or time-based delayed cord clamping (TBCC), stratified by gestational age and treatment center. Infants receiving PBCC were stabilised with umbilical cord intact, which was clamped after reaching cardiorespiratory stability (heart rate >100 bpm and SpO2 >85% while supplemental oxygen <40%). In TBCC the cord was clamped after 30-60 s. The primary outcome was survival without major cerebral injury and/or necrotizing enterocolitis. The primary and key secondary analyses were done in both the intention-to-treat and per-protocol populations. The trial was registered with ClinicalTrials.gov (NCT03808051).
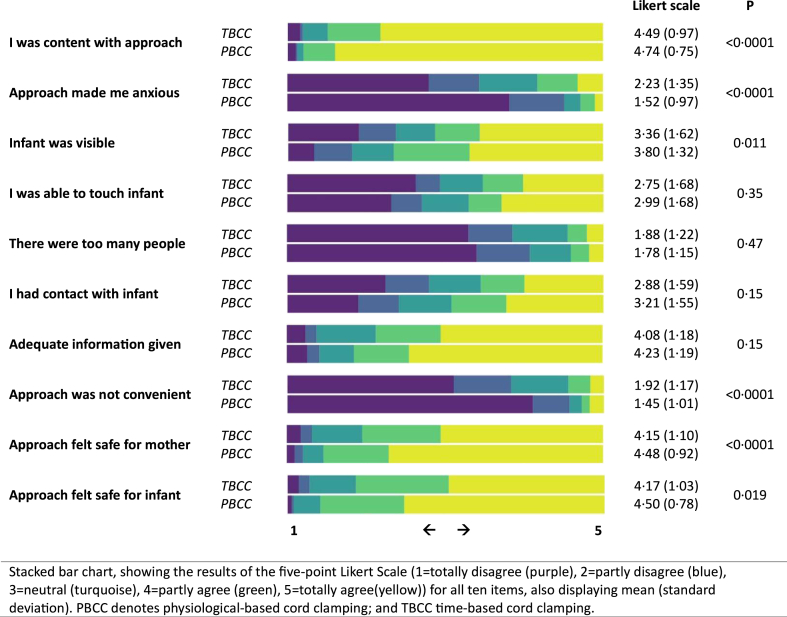
Findings: From January 25, 2019, through October 2, 2022, 669 infants were randomised (median gestational age 27+5 weeks (IQR 26+2-28+6)) and included in the intention-to-treat population. Intact survival occurred in 241 of 339 infants (71.1%) after PBCC, compared with 223 of 330 (67.6%) after TBCC (odds ratio 1.18, 95% CI 0.84-1.66; absolute risk difference 3.1 %points, 95% CI -11.0 to 15.8, p = 0.33). Pre-specified subgroup analysis showed 69.9% intact survival in male infants after PBCC, compared with 61.8% after TBCC (odds ratio 2.32, 95% CI 1.42-3.78, p for interaction 0.026). Secondary outcomes showed fewer red blood cell transfusions after PBCC (rate ratio 0.83, 95% CI 0.75-0.92, p = 0.0003), lower incidence of late-onset sepsis (27.4% versus 33.3%, odds ratio 0.77, 95% CI 0.62-0.95, p = 0.013) and lower admission temperature (36.3 °C versus 36.7 °C, mean difference -0.5, 95% CI -0.8 to -0.3, p < 0.0001). Parents were less anxious (Likert scale 1.52 (SD 0.97) versus 2.23 (SD 1.35); p < 0.001) and more content (Likert scale 4.74 (SD 0.75) versus 4.49 (SD 0.97); p < 0.001) after PBCC.
Interpretation: PBCC in very preterm infants did not increase survival without major cerebral injury or necrotizing enterocolitis compared to TBCC in the entire cohort. A possible beneficial effect in male infants requires confirmation from other trials. PBCC was safe to perform and parents reported more contentment and less anxiety.
Funding: The Netherlands Organization for Health Research and Development.
Keywords: Cord clamping; Newborn resuscitation; Preterm infants.
© 2024 The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests. The equipment used in this trial was either designed and built by Leiden University Medical Center (for 3 participating centers) or purchased from Concord Neonatal B.V. (Leiden, The Netherlands). ABtP, SBH, and AHvK are unpaid members of the Scientific Advisory Board of Concord Neonatal B.V. Authors do not have financial relationship with or support from Concord Neonatal. LUMC is owner of the invention and has a license agreement with Concord neonatal, for which LUMC receives royalties. LUMC has the policy to allocate and divide the amount received among the hospital, department and inventors. AtP is one of the inventors. The company had no role in the design of the study; in the collection, analysis, or interpretation of data; or in the writing of the manuscript. MJV is an unpaid board member of the Dutch neonatal patient and parent society Care4Neo.
Figures
References
-
- Fogarty M., Osborn D.A., Askie L., et al. Delayed vs early umbilical cord clamping for preterm infants: a systematic review and meta-analysis. Am J Obstet Gynecol. 2018;218(1):1–18. - PubMed
-
- Seidler A.L., Aberoumand M., Hunter K.E., et al. Deferred cord clamping, cord milking, and immediate cord clamping at preterm birth: a systematic review and individual participant data meta-analysis. Lancet. 2023;402(10418):2209–2222. - PubMed
-
- Aziz K., Lee H.C., Escobedo M.B., et al. Part 5: neonatal resuscitation: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142(16_suppl_2):S524–S550. - PubMed
-
- Madar J., Roehr C.C., Ainsworth S., et al. European Resuscitation Council guidelines 2021: newborn resuscitation and support of transition of infants at birth. Resuscitation. 2021;161:291–326. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
