

When to stop immunotherapy for advanced melanoma: the emulated target trials
- PMID: 39717261
- PMCID: PMC11664069
- DOI: 10.1016/j.eclinm.2024.102960
When to stop immunotherapy for advanced melanoma: the emulated target trials
Abstract
Background: Immune checkpoint inhibitors (ICIs) have demonstrated their efficacy with a 7.5-year overall survival (OS) close to 50% for advanced stages. The design of clinical trials provides for treatment until progression or toxicity, or for a maximum duration of two years. Prolonged follow-up of responders after treatment cessation shows sustained response and a low risk of relapse in the months following cessation. To date, the optimal duration of anti-PD-1 therapy for metastatic melanoma remains unestablished. The objective of this work was to evaluate the optimal duration of ICI administration.
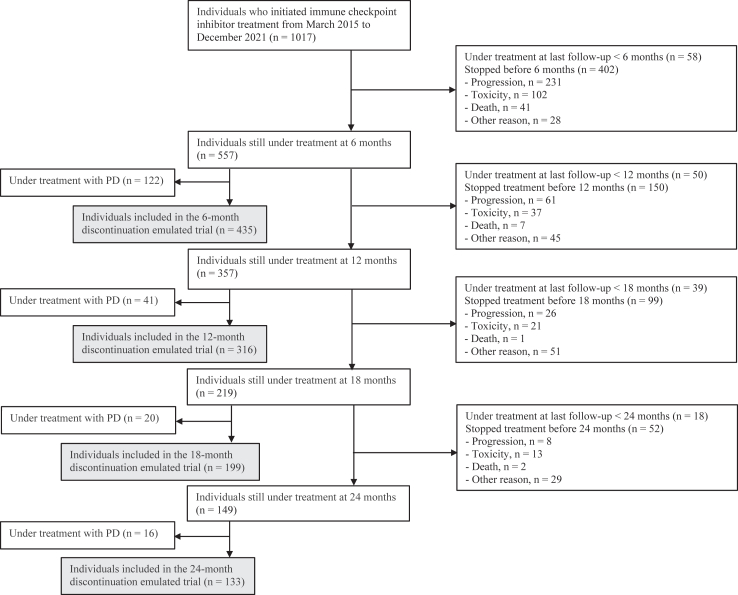
Methods: We emulated target trials using the cloning, weighting and censoring approach. Each emulation trial aimed to compare the effect of discontinuing versus continuing ICIs at a specific timepoint, among patients still under treatment and with disease control at that time. Patients were from MelBase between 2015 and 2021.
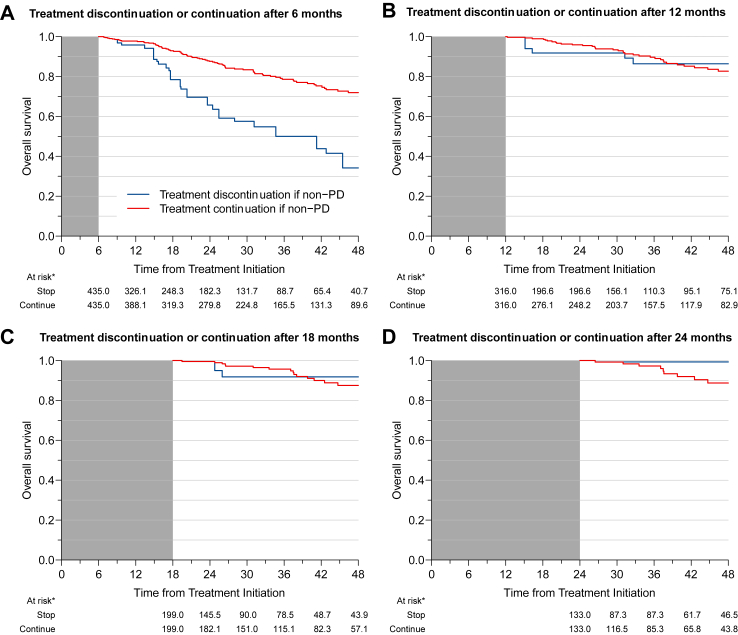
Findings: 435 participants in the MelBase cohort were eligible and were included in the 6-month discontinuation emulated trial. The results showed significantly lower OS when treatment was discontinued, than when treatment was prolonged for at least three months. The 48-month survival difference was 37.8% (95% confidence interval [CI] 19.8-60.5), and the corresponding restricted mean survival time difference was 8.3 months (95% CI: 4.1-12.7). Neither the 12-month nor the 18-month discontinuation emulated trials showed evidence of benefit of either discontinuing or continuing ICIs at either of these timepoints. The 24-month discontinuation emulated trial results were more in favor of discontinuing than continuing treatment at that time point, with an absolute 48-month survival rate that was 10.5% higher (95% CI 4.4-18.1).
Interpretation: These results suggest that a one-year course of immunotherapy is both necessary and sufficient for patients with advanced melanoma. Prolonged treatment beyond 2 years does not appear to be beneficial in terms of survival and could even be detrimental.
Funding: This work was supported by a grant from Bristol Myers Squibb, Merck Sharp Dhome, Pierre Fabre, Novartis, Sun Pharm, Regeneron, Sanofi, Nektar, Therapeutics and Oncyte.
Keywords: Advanced melanoma; Duration of treatment; Emulated trial; Immunotherapy.
© 2024 The Authors.
Conflict of interest statement
LM reports advisory board and travel expenses from Bristol Myers Squibb, Merck Sharp and Dhome, Pierre Fabre, Novartis and Sun Pharm. SD reports advisory board and travel expenses from Bristol Myers Squibb and Merck Sharp, and Dhome; research fundings from Bristol Myers Squibb, Merck Sharp and Dhome, and Pierre Fabre. FBP reports financial support outside the submitted work from Bristol Myers Squibb, Merck Sharp and Dhome, Pierre Fabre and Novartis. JDQ reports advisory board from Merck Sharp and Dhome, Pierre Fabre, Novartis and Bristol Myers Squibb. CGM reports advisory board and travel expenses from Pierre Fabre, Bristol Myers Squibb and Merck Sharp and Dhome. PS reports advisory board and travel expenses from Bristol Myers Squibb, Merck Sharp and Dhome and Pierre Fabre and Novartis; consulting fees from Bristol Myers Squibb, Merck Sharp and Dhome, Pierre Fabre, Regeneron, Sanofi, Damae and Novartis. TL reports advisory board and travel expenses from Bristol Myers Squibb, Merck Sharp and Dhome, Pierre Fabre and Novartis. HM reports advisory board from Pierre Fabre, Bristol Myers Squibb, Merck Sharp and Dhome, Novartis, Regeneron and Sun Pharma; research funding from Pierre Fabre, Bristol Myers Squibb, Merck Sharp and Dhome, Novartis, Regeneron, Nektar Therapeutics, 4SC and Incyte; and research grant from Leo Pharma and Merck Sharp and Dhome. All other authors declare no completing interests.
Figures

References
-
- Eggermont A.M.M., Blank C.U., Mandala M., et al. Follow-up confirms recurrence-free survival benefit of adjuvant pembrolizumab in high-risk stage III melanoma: updated results from the EORTC 1325-MG/KEYNOTE-054 trial. J Clin Oncol. 2020;38(33):3925–3936. doi: 10.1200/JCO.20.02110. Epub 2020 Sep 18. PMID: 32946353; PMCID: PMC7676886. - DOI - PMC - PubMed
-
- Ascierto P.A., Del Vecchio M., Mandalá M., et al. Adjuvant nivolumab versus ipilimumab in resected stage IIIB-C and stage IV melanoma (CheckMate 238): 4-year results from a multicentre, double-blind, randomised, controlled, phase 3 trial. Lancet Oncol. 2020;21(11):1465–1477. doi: 10.1016/S1470-2045(20)30494-0. Epub 2020 Sep 19. Erratum in: Lancet Oncol. 2021 Oct;22(10):e428. PMID: 32961119. - DOI - PubMed
-
- Luke J.J., Rutkowski P., Queirolo P., et al. Pembrolizumab versus placebo as adjuvant therapy in completely resected stage IIB or IIC melanoma (KEYNOTE-716): a randomised, double-blind, phase 3 trial. Lancet. 2022;399(10336):1718–1729. doi: 10.1016/S0140-6736(22)00562-1. Epub 2022 Apr 1. PMID: 35367007. - DOI - PubMed
LinkOut - more resources
Full Text Sources
