

MRI-Based Morphometric Comparison of Lower Leg Muscles and Tendons in Individuals With Medial Tibial Stress Syndrome
- PMID: 39717266
- PMCID: PMC11666316
- DOI: 10.1155/bmri/8827692
MRI-Based Morphometric Comparison of Lower Leg Muscles and Tendons in Individuals With Medial Tibial Stress Syndrome
Abstract
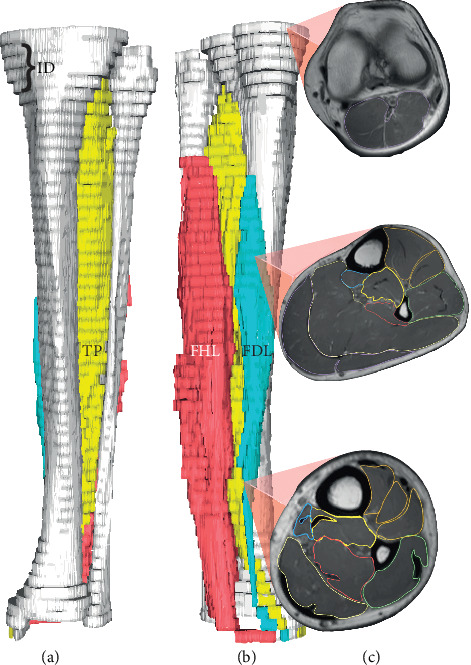
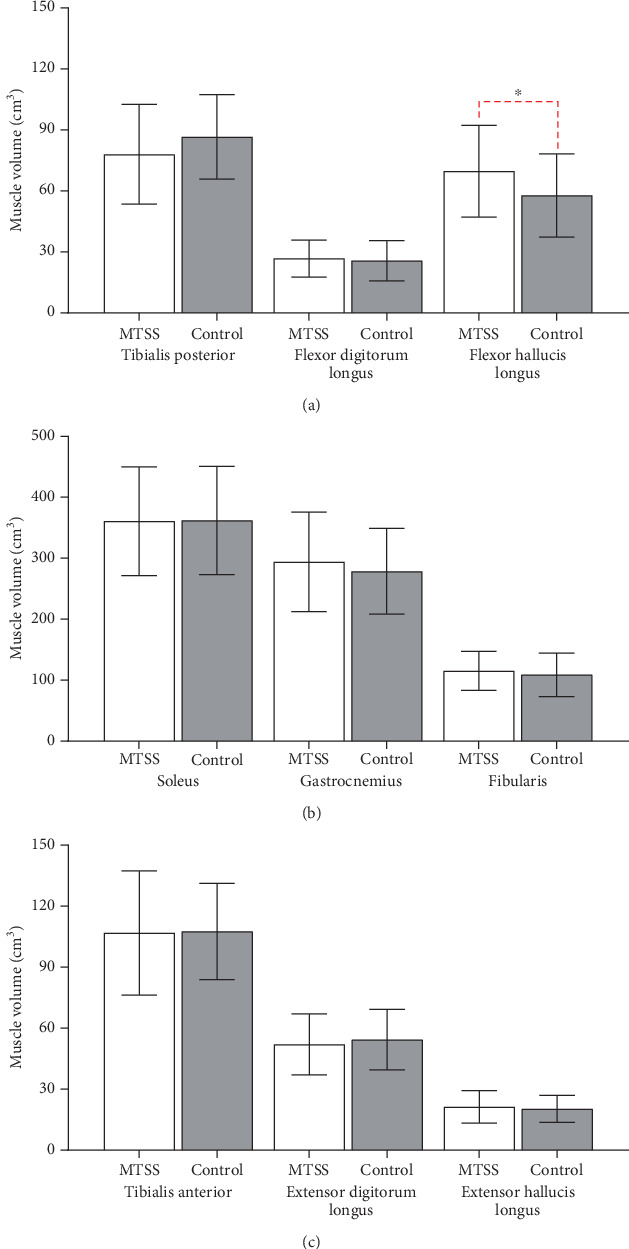
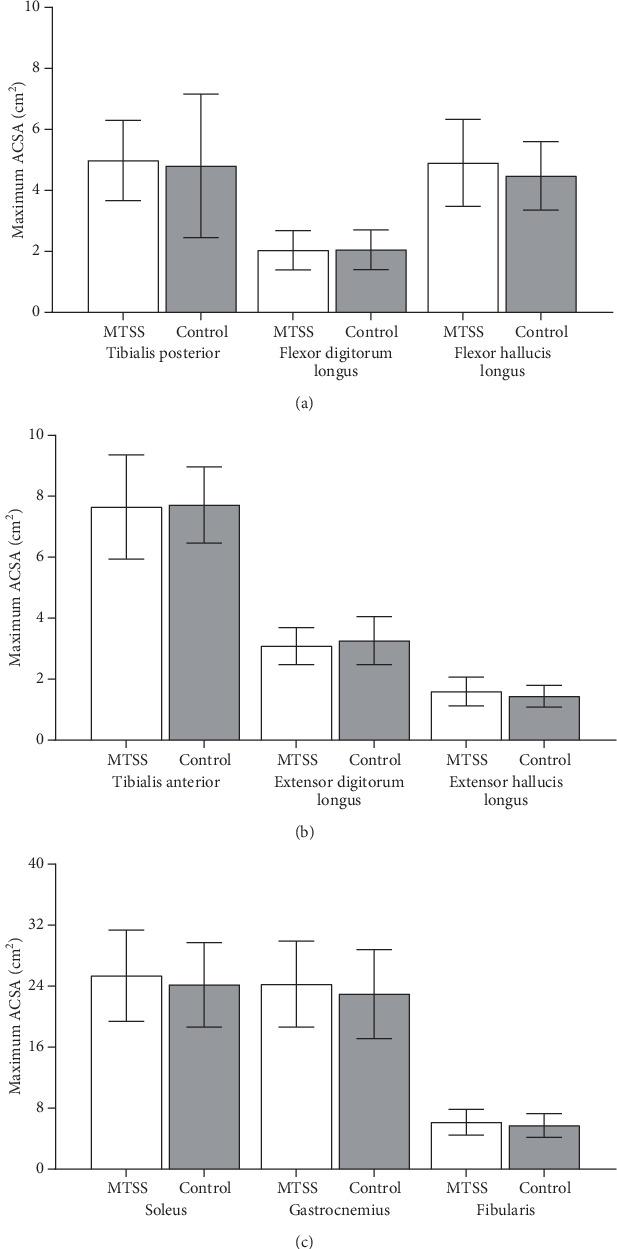
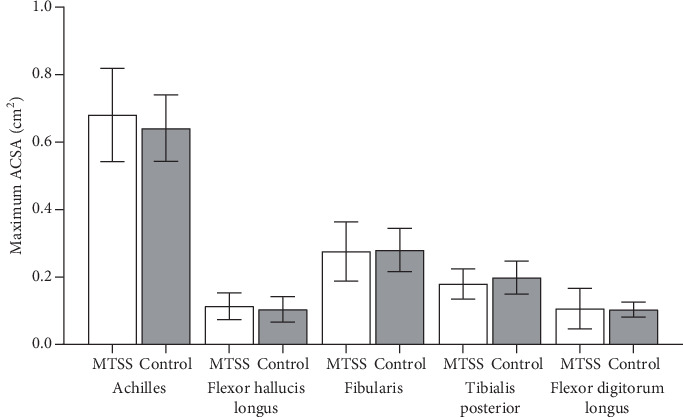
Runners frequently suffer from medial tibial stress syndrome (MTSS), often linked to excessive eccentric muscle contractions causing periosteal traction by the muscles in the deep posterior compartment. However, the effects of MTSS on these muscles and tendons remain underexplored. This study is aimed at investigating changes in muscle and tendon volumes in this compartment, as well as cross-sectional area measurements, using magnetic resonance imaging. Thirty individuals were divided into two groups: MTSS (n = 18; mean age 30.3 ± 12.4) and control (n = 12; age 35.2 ± 9.2). The anterior, deep posterior, superficial posterior, and lateral compartment muscles, along with their respective tendons, were compared between groups, and possible sex differences were also evaluated. The deep posterior compartment showed a significant volume difference of 0.41 cm3/kg3/4 in the MTSS group (p = 0.034), primarily due to the flexor hallucis longus (FHL), which had a 0.55 cm3/kg3/4 greater normalized volume (17.12% greater mean muscle volume) compared to controls (p = 0.023; Cohen d = 0.895). No association between sex and MTSS was found (p = 0.752). In conclusion, the FHL muscle exhibited increased normalized volume in the MTSS group compared to controls, with no sex-related differences in MTSS. Clinicians should consider the assessment of FHL muscle volume in routine evaluations of patients presenting with symptoms suggestive of MTSS.
Keywords: MRI; MTSS; deep posterior compartment; flexor hallucis longus; muscle volume.
Copyright © 2024 Lucas Nogueira de Oliveira et al.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Menéndez C., Batalla L., Prieto A., Rodríguez M. Á., Crespo I., Olmedillas H. Medial tibial stress syndrome in novice and recreational runners: a systematic review. International Journal of Environmental Research and Public Health . 2020;17(20):p. 7457. doi: 10.3390/ijerph17207457. - DOI - PMC - PubMed
-
- Ramskov D., Rasmussen S., Sørensen H., Parner E. T., Lind M., Nielsen R. Progression in running intensity or running volume and the development of specific injuries in recreational runners: run clever, a randomized trial using competing risks. The Journal of Orthopaedic and Sports Physical Therapy . 2018;48(10):740–748. doi: 10.2519/jospt.2018.8062. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
