

Association of cardiovascular-kidney-metabolic index with all-cause mortality during hospitalization in critically ill patients: a retrospective cohort study from MIMIC IV2.2
- PMID: 39717440
- PMCID: PMC11663873
- DOI: 10.3389/fcvm.2024.1513212
Association of cardiovascular-kidney-metabolic index with all-cause mortality during hospitalization in critically ill patients: a retrospective cohort study from MIMIC IV2.2
Abstract
Background: The cardiovascular-kidney-metabolic index (CKMI), a novel functional indicator proposed in this study, aims to accurately reflect the functional status of the heart, kidneys, and metabolism. However, its ability to predict mortality risk in critically ill patients during their stay in the intensive care unit (ICU) remains uncertain. Therefore, this study aims to validate the correlation between the CKMI during hospitalization and all-cause mortality.
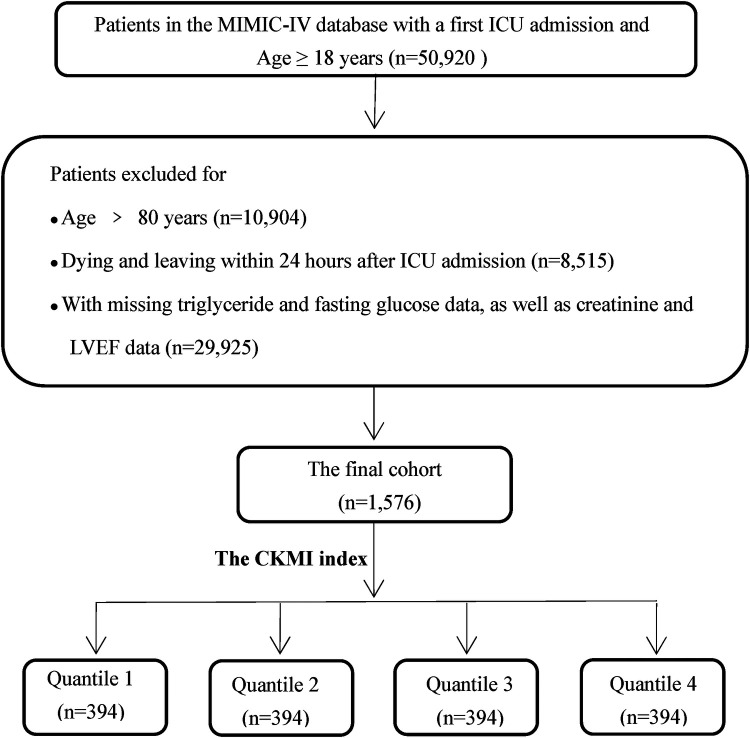
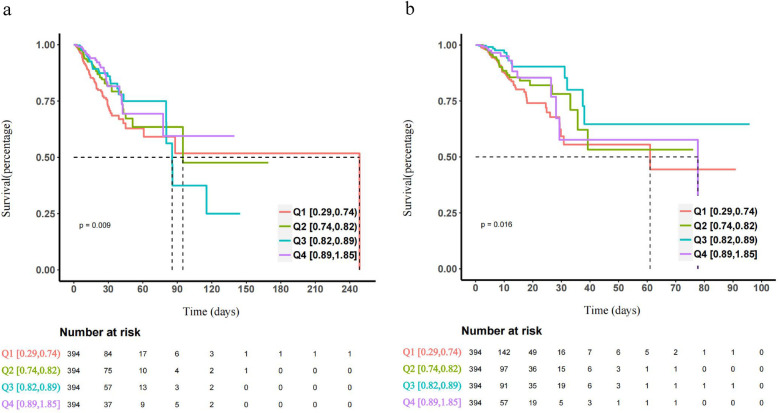
Methods: The study utilized the Medical Information Mart for Intensive Care IV 2.2 (MIMIC-IV) dataset for a retrospective analysis of cohorts. The cohorts were divided into quartiles based on CKMI index levels. The primary endpoint was all-cause mortality during ICU and hospital stay, while secondary endpoints included the duration of ICU stay and overall hospitalization period. We established Cox proportional hazards models and employed multivariable Cox regression analysis and restricted cubic spline (RCS) regression analysis to explore the relationship between CKMI index and all-cause mortality during hospitalization in critically ill patients. Additionally, subgroup analyses were conducted based on different subgroups.
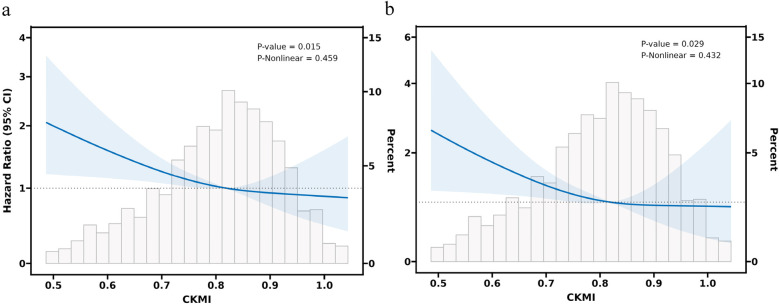
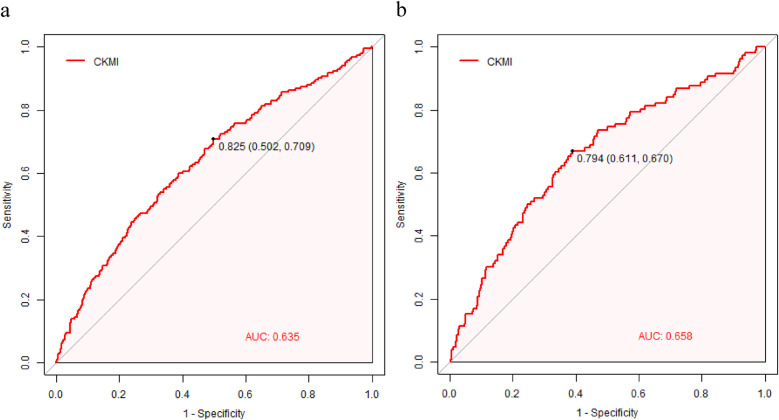
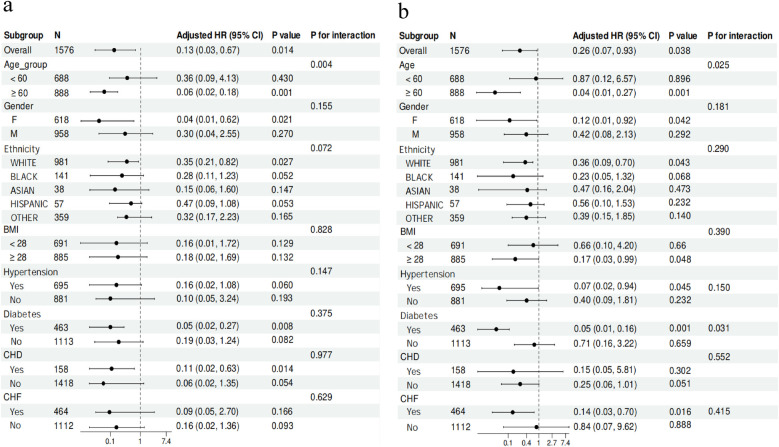
Results: The study enrolled 1,576 patients (male 60.79%). In-patient and ICU mortality was 11.55% and 6.73%. Multivariate COX regression analysis demonstrated a significant negative correlation between CKMI index and the risk of hospital death [HR, 0.26 (95% CI 0.07-0.93), P = 0.038] and ICU mortality [HR, 0.13 (95% CI 0.03-0.67), P = 0.014].RCS regression model revealed that in-hospital mortality (P-value =0.015, P-Nonlinear =0.459) and ICU mortality (P-value =0.029, P-Nonlinear =0.432) increased linearly with increasing CKMI index. Subgroup analysis confirmed consistent effect size and direction across different subgroups, ensuring stable results.
Conclusion: Our research findings suggest that a higher CKMI index is associated with a significant reduction in both in-hospital and ICU mortality among critically ill patients. Therefore, CKMI index emerges as a highly valuable prognostic indicator for predicting the risk of in-hospital death in this population. However, to strengthen the validity of these results, further validation through larger-scale prospective studies is imperative.
Keywords: MIMIC-IV database; cardiovascular-kidney-metabolic index; in-hospital mortality; intensive care unit; retrospective cohort study.
© 2024 Qu, Liu, Nie and Huang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
A retrospective study utilized MIMIC-IV database to explore the potential association between triglyceride-glucose index and mortality in critically ill patients with sepsis.Sci Rep. 2024 Oct 15;14(1):24081. doi: 10.1038/s41598-024-75050-8. Sci Rep. 2024. PMID: 39402158 Free PMC article.
-
Association between the TyG index and the risk of in-hospital mortality from early sepsis-related acute kidney injury in critically ill patients: a secondary analysis of MIMIC-IV 2008-2022.BMJ Open. 2025 May 7;15(5):e099529. doi: 10.1136/bmjopen-2025-099529. BMJ Open. 2025. PMID: 40341153 Free PMC article.
-
Correlation between serum phosphate and all-cause mortality in critically ill patients with coronary heart disease accompanied by chronic kidney disease: a retrospective study using the MIMIC-IV database.Front Cardiovasc Med. 2024 May 31;11:1371000. doi: 10.3389/fcvm.2024.1371000. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38883990 Free PMC article.
-
Association between triglyceride-glucose index and in-hospital mortality in critically ill patients with sepsis: analysis of the MIMIC-IV database.Cardiovasc Diabetol. 2023 Nov 8;22(1):307. doi: 10.1186/s12933-023-02041-w. Cardiovasc Diabetol. 2023. PMID: 37940931 Free PMC article.
-
Association of dynamic change of triglyceride-glucose index during hospital stay with all-cause mortality in critically ill patients: a retrospective cohort study from MIMIC IV2.0.Cardiovasc Diabetol. 2023 Jun 17;22(1):142. doi: 10.1186/s12933-023-01874-9. Cardiovasc Diabetol. 2023. PMID: 37330498 Free PMC article.
References
-
- Zampieri FG, Serpa-Neto A, Wald R, Bellomo R, Bagshaw SM. Hierarchical endpoints in critical care: a post-hoc exploratory analysis of the standard versus accelerated initiation of renal-replacement therapy in acute kidney injury and the intensity of continuous renal- replacement therapy in critically ill patients trials. J Crit Care. (2024) 82:154767. 10.1016/j.jcrc.2024.154767 - DOI - PubMed
-
- Yan F, Chen X, Quan X, Wang L, Wei X, Zhu J. Association between the stress hyperglycemia ratio and 28-day all-cause mortality in critically ill patients with sepsis:a retrospective cohort study and predictive model establishment based on machine learning. Cardiovasc Diabetol. (2024) 23:163. 10.1186/s12933-024-02265-4 - DOI - PMC - PubMed
-
- Cheng L, Zhang F, Xue W, Yu P, Wang X, Wang H, et al. Association of dynamic change of triglyceride-glucose index during hospital stay with all-cause mortality in critically ill patients: a retrospective cohort study from mimic iv2.0. Cardiovasc Diabetol. (2023) 22:142. 10.1186/s12933-023-01874-9 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources