

Hepatocellular carcinoma hosts cholinergic neural cells and tumoral hepatocytes harboring targetable muscarinic receptors
- PMID: 39717507
- PMCID: PMC11663970
- DOI: 10.1016/j.jhepr.2024.101245
Hepatocellular carcinoma hosts cholinergic neural cells and tumoral hepatocytes harboring targetable muscarinic receptors
Abstract
Background & aims: Owing to unexplained interpatient variation and treatment failure in hepatocellular carcinoma (HCC), novel therapeutic approaches remain an urgent clinical need. Hepatic neurons, belonging to the autonomic nervous system (ANS), mediate liver/whole body crosstalk. Pathological innervation of the ANS has been identified in cancer, nurturing tumor stroma and conferring stronger carcinogenic properties.
Methods: We characterized the innervation of liver tumors from the French Liver Biobank, then applied bioinformatics to TCGA (The Cancer Genome Atlas), several other datasets and a European validation cohort, to re-evaluate patient stratification. Cell biology and pharmacology studies were also performed.
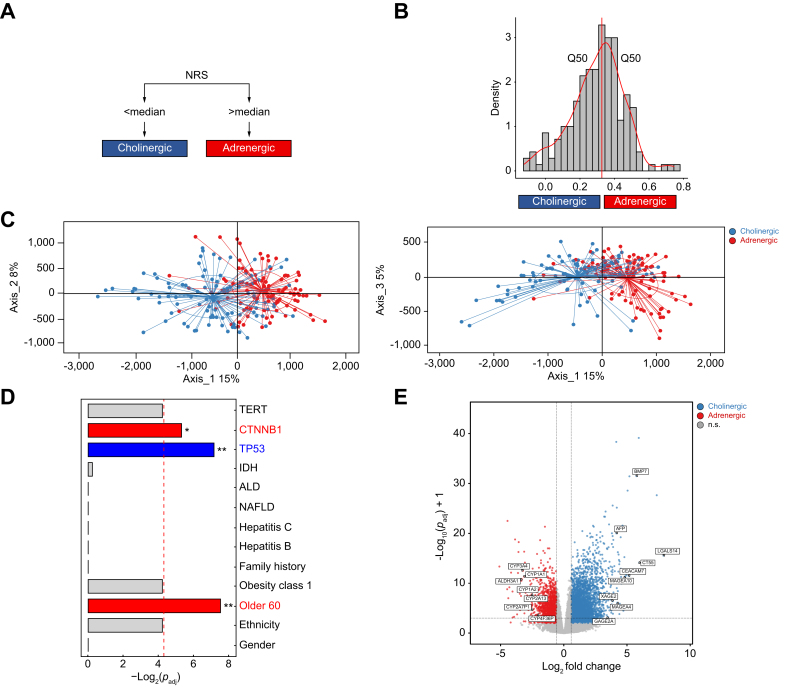
Results: Densely packed nucleated DCX+, synaptophysin+, NeuN+, VAChT+, TH-, CD31-, CD45- clusters, to date undetected, were identified in human HCCs, and independently confirmed by single-cell RNA sequencing data. Using the new concept of a neuronal score, human and rat HCCs displayed tightly netrin-1-associated neural reconfiguration towards cholinergic polarity, which was associated with chronic liver disease progression, cancer onset and many features of aggressive (proliferative class) HCC, including shortened survival. This score was conditioned by tumoral hepatocytes, and predicted sorafenib efficacy in the STORM HCC phase III trial. Conversely, intratumoral adrenergic lymphocytes were enriched in TEMRA and cytotoxic phenotypes. Amongst all cholinergic transcripts, the medically targeted CHRM3 receptor was enriched and associated with pathogenic traits in HCC, as well as poor prognosis in HCC stages 1-2, while its level dropped upon experimental re-differentiation. Its pharmacological inhibition with low concentrations of anticholinergic drugs, but not cholinomimetics, decreased anchorage-independent growth and anoikis, synergized with sorafenib and lenvatinib in HCC class 1 to 3 lines, yet not in primary human hepatocytes, and preserved mature hepatocyte functions.
Conclusion: These data identify cholinergic processes as instrumental in liver carcinogenesis and support the use of EMA/FDA-approved cholinergic drugs in HCC research.
Impact and implications: Hepatocellular carcinoma (HCC) care has long been hampered by the enigmatic nature of disease evolution, as well as of response or resistance to treatment. Hepatic neurons are likely the least studied liver cell type and mediate patients singularities from the ANS to the organ in real-time. Cholinergic inputs identified in this study as pathogenic may be targeted with the well charted pharmacopoeia of neurotropic drugs already available, for basic or clinical research purposes, with an expected high level of safety.
Keywords: HCC; M3 muscarinic receptor; TKI resistance; autonomic nervous system; cholinergic; neuronal score; scRNA-seq; spheroids; synergy; transcriptomics.
© 2024 The Author(s).
Conflict of interest statement
Research Support to JML: Bayer Pharmaceuticals, Eisai Inc, Bristol-Myers Squibb and Ipsen. Consultancy (JML): Bayer HealthCare Pharmaceuticals, Eisai Inc, Merck, Bristol-Myers Squibb, Eli Lilly, Roche, Genentech, Ipsen, Glycotest, AstraZeneca, Omega Therapeutics, Mina Alpha, Boston Scientific, Exelixis, Bluejay, Captor Therapeutics. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures








References
-
- Llovet J.M., Kelley R.K., Villanueva A., et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7:6. - PubMed
-
- Llovet J.M., Montal R., Sia D., et al. Molecular therapies and precision medicine for hepatocellular carcinoma. Nat Rev Clin Oncol. 2018;15:599–616. - PubMed
-
- Zeldovich L., Manish V. Cold Spring Harbor Stories and Media; 2022 Aug 22. Cancer has a lot of nerve.
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
