

Significant differences in knee kinematics of healthy subjects with high and low anterior tibial laxity
- PMID: 39717532
- PMCID: PMC11664222
- DOI: 10.3389/fbioe.2024.1514516
Significant differences in knee kinematics of healthy subjects with high and low anterior tibial laxity
Abstract
Background: Anterior tibial laxity is considered to be a risk factor for knee injuries, including anterior cruciate ligament ruptures. The anterior cruciate ligament reconstruction also aims to restore anterior tibial laxity. While anterior tibial laxity is considered to be linked to dynamic knee stability, the mechanisms connecting anterior tibial laxity to these stability issues are not fully understood. The purpose of this study was to investigate the kinematic alterations between different anterior tibial laxity in healthy subjects. We hypothesized that anterior tibial laxity affects the anteroposterior tibial displacement during dynamic movements.
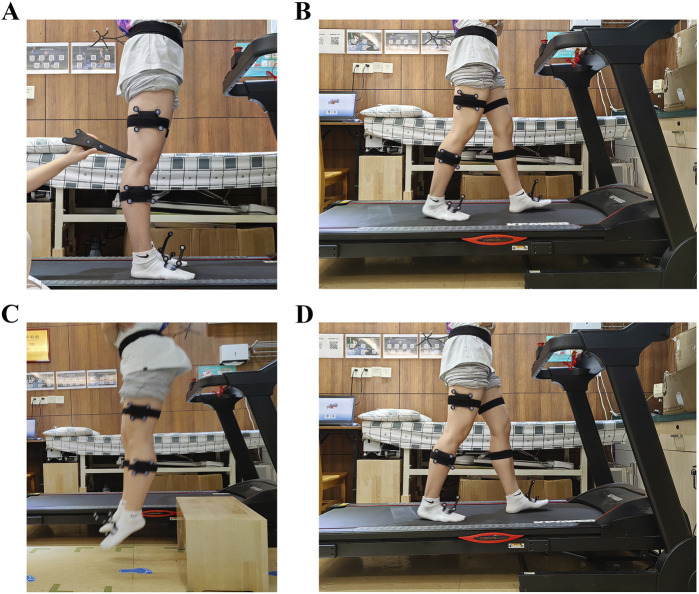
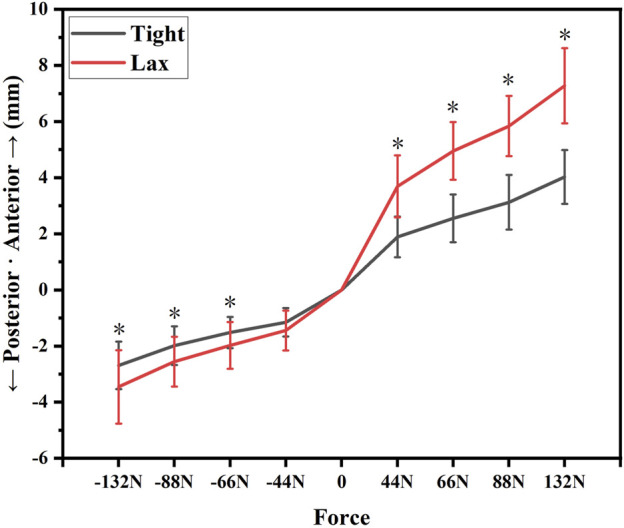
Methods: This study involved thirty-five healthy subjects. There were twenty males and fifteen females with an average age of 18.91 ± 0.78 years. Their knees were categorized into "Tight" (the smallest 50%) and "Lax" (the largest 50%) groups based on anterior tibial laxity measurements using a Kneelax3 arthrometer. Kinematic data were collected using a three-dimensional motion capture system when they performed level walking, upslope walking, and vertical jumping. The knee kinematics were recorded for statistical analysis. We used independent sample t-tests to analyze key kinematic differences between groups.
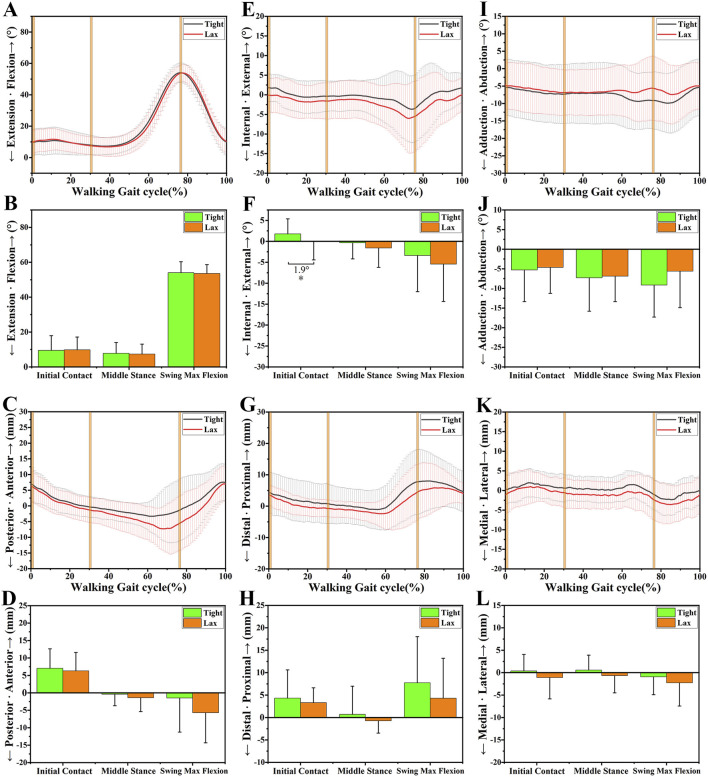
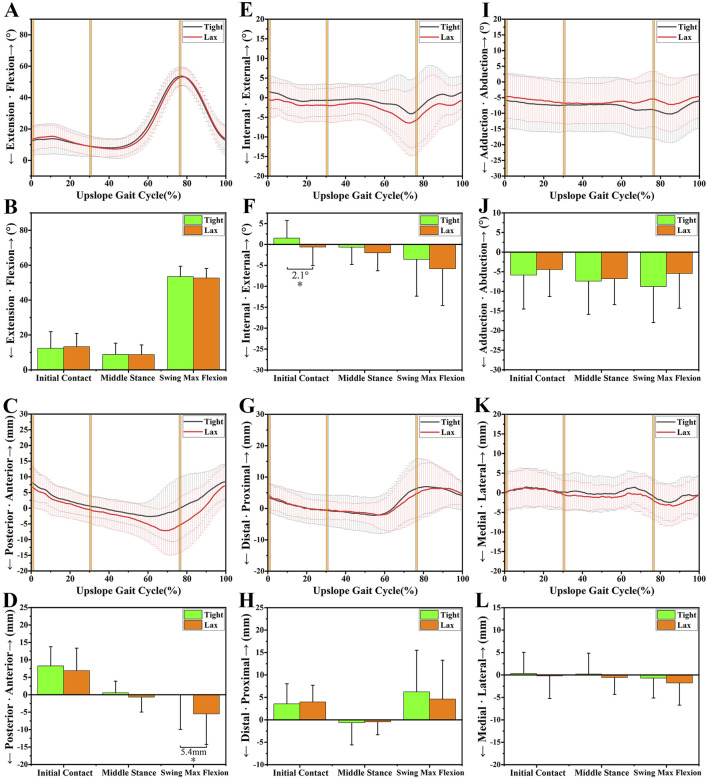
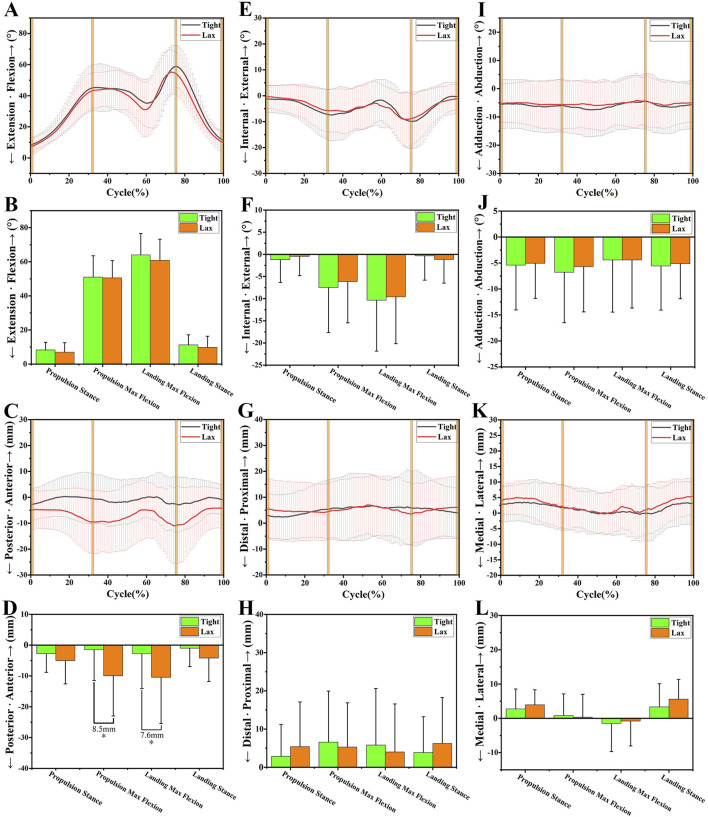
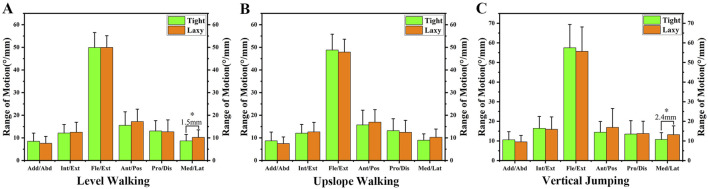
Results: The "Lax" group exhibited increased posterior tibial translation during upslope walking (5.4 ± 2.22 mm at swing max flexion, p = 0.018) and vertical jumping (8.5 ± 2.78 mm at propulsion max flexion, p = 0.003; 7.6 ± 3.17 mm at landing max flexion, p = 0.019) than the "Tight" group. Significant differences in tibial internal rotation were observed during initial contact of the gait cycle of level walking (1.9° ± 0.95°, p = 0.049) and upslope walking (2.1° ± 1.03°, p = 0.041) in the "Lax" group compared to the "Tight" group. No significant differences in adduction/abduction or medial/lateral tibial translation were found between groups.
Conclusion: The study revealed that high anterior tibial laxity resulted in increased posterior tibial translation and tibial internal rotation. High anterior tibial laxity resulted in dynamic instability of knees during motions, especially in high-demanding activities like upslope or vertical jumping. However, further research is needed to explore the clinical functional effects of knee laxity.
Keywords: anterior tibial laxity; dynamic stability; kinematic alterations; knee; knee kinematics.
Copyright © 2024 Chen, Chen, Kang, Lin, Zheng, Liu, Guo, Li, Lin and Zeng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Abulhasan J. F., Grey M. J. (2017). Anatomy and physiology of knee stability. J. Funct. Morphol. Kinesiol 2, 34. 10.3390/jfmk2040034 - DOI
-
- Boeth H., Duda G. N., Heller M. O., Ehrig R. M., Doyscher R., Jung T., et al. (2013). Anterior cruciate ligament–deficient patients with passive knee joint laxity have a decreased range of anterior-posterior motion during active movements. Am. J. Sports Med. 41, 1051–1057. 10.1177/0363546513480465 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous