

European Society for Gynaecological Endoscopy (ESGE) Good Practice Recommendations on surgical techniques for Removal of Fibroids: Part 2 Hysteroscopic Myomectomy
- PMID: 39718323
- PMCID: PMC11819789
- DOI: 10.52054/FVVO.16.4.054
European Society for Gynaecological Endoscopy (ESGE) Good Practice Recommendations on surgical techniques for Removal of Fibroids: Part 2 Hysteroscopic Myomectomy
Abstract
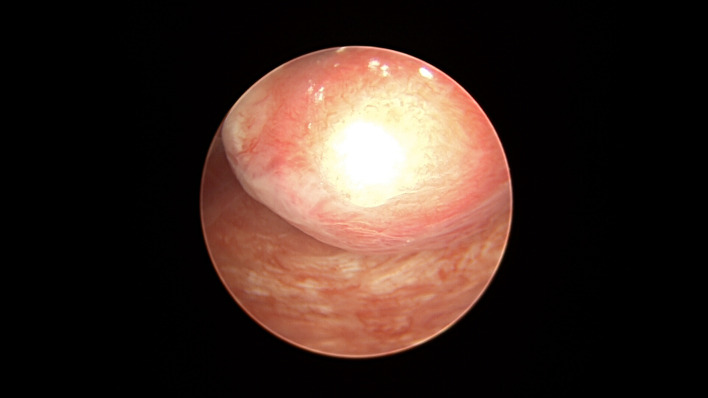
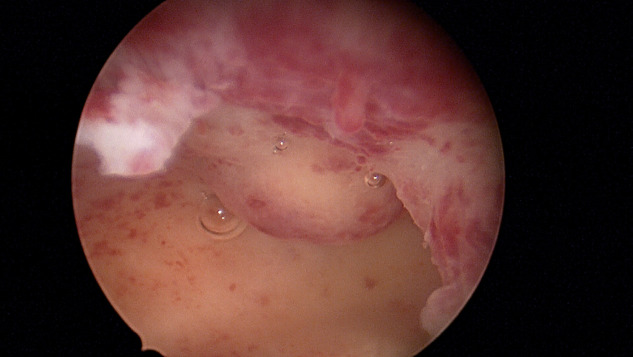
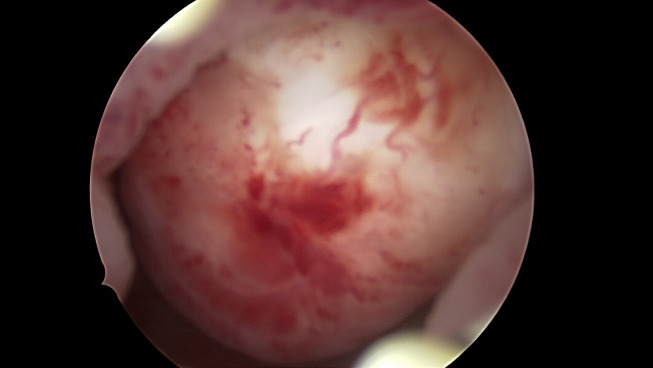
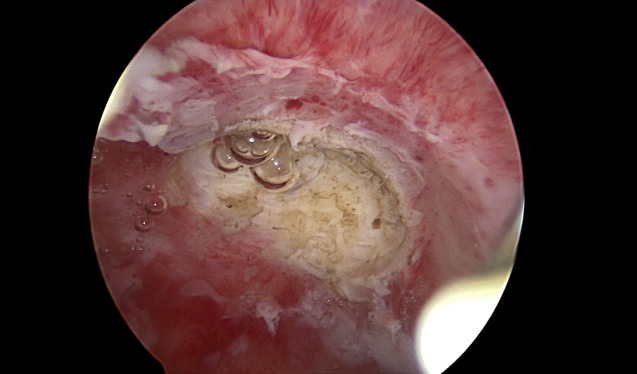
Submucosal uterine fibroids are the rarest type of fibroids. They can lead to abnormal uterine bleeding and may play a role in infertility and miscarriage. Hysteroscopic myomectomy is the preferred treatment to relieve bleeding caused by these fibroids and to restore the normal structure of the uterine cavity. The European Society for Gynaecological Endoscopy Uterine Fibroids Working Group developed recommendations based on the best available evidence and expert opinion for the surgical treatment of uterine fibroids. In this second part of the recommendations, hysteroscopic approaches are described. This review explores the techniques related to hysteroscopic myomectomy, focusing on narrower scopes, fluid management and advances in tissue removal systems and electrosurgery.
Figures



Similar articles
-
European Society for Gynaecological Endoscopy (ESGE) Good Practice Recommendations on surgical techniques for removal of fibroids: part 1 abdominal (laparoscopic and open) myomectomy.Facts Views Vis Obgyn. 2024 Sep;16(3):263-280. doi: 10.52054/FVVO.16.3.041. Facts Views Vis Obgyn. 2024. PMID: 39357857 Free PMC article.
-
Hysteroscopic myomectomy for submucosal type 2 fibroids with cold enucleation technique and complete fibroid extraction using a double-lumen intracervical cannula.Fertil Steril. 2021 Feb;115(2):522-524. doi: 10.1016/j.fertnstert.2020.09.028. Epub 2020 Dec 4. Fertil Steril. 2021. PMID: 33272627
-
HYSTEROSCOPIC MYOMECTOMY.Medicina (Kaunas). 2022 Nov 11;58(11):1627. doi: 10.3390/medicina58111627. Medicina (Kaunas). 2022. PMID: 36422166 Free PMC article. Review.
-
The management of uterine fibroids in women with otherwise unexplained infertility.J Obstet Gynaecol Can. 2015 Mar;37(3):277-285. doi: 10.1016/S1701-2163(15)30318-2. J Obstet Gynaecol Can. 2015. PMID: 26001875
-
Hysteroscopic myomectomy: a comparison of techniques and review of current evidence in the management of abnormal uterine bleeding.Curr Opin Obstet Gynecol. 2018 Aug;30(4):243-251. doi: 10.1097/GCO.0000000000000475. Curr Opin Obstet Gynecol. 2018. PMID: 29939852 Review.
Cited by
-
Feasibility of single step hysteroscopic myomectomy: fibroid size is the most significant factor based on data from a single centre and surgeon.Facts Views Vis Obgyn. 2025 Jun 27;17(2):110-120. doi: 10.52054/FVVO.2025.10. Epub 2025 May 27. Facts Views Vis Obgyn. 2025. PMID: 40423569 Free PMC article.
References
-
- AAGL Advancing Minimally Invasive Gynecology Worldwide, Munro MG, Storz K, et al. AAGL Practice Report: Practice Guidelines for the Management of Hysteroscopic Distending Media: (Replaces Hysteroscopic Fluid Monitoring Guidelines. J Am Assoc Gynecol Laparosc. 2000;7:167-168.) J Minim Invasive Gynecol. 2013;20:137–148. - PubMed
-
- AAGL. AAGL Practice Report: Practice Guidelines for the Diagnosis and Management of Submucous Leiomyomas. J Minim Invasive Gynecol. 2012;19:152–171. - PubMed
-
- Agostini A, Cravello L, Shojai R, et al. Postoperative infection and surgical hysteroscopy. Fertil Steril. 2002;77:766–768. - PubMed
-
- Bettocchi S, Ceci O, Di Venere R, et al. Advanced operative office hysteroscopy without anaesthesia: analysis of 501 cases treated with a 5 Fr. bipolar electrode. Hum Reprod. 2002;17:2435–2438. - PubMed
LinkOut - more resources
Full Text Sources