

IL-1β primed mesenchymal stromal cells moderate hemorrhagic shock-induced vascular permeability
- PMID: 39719575
- PMCID: PMC11668119
- DOI: 10.1186/s12967-024-05961-7
IL-1β primed mesenchymal stromal cells moderate hemorrhagic shock-induced vascular permeability
Abstract
Background: Hemorrhagic shock (HS) corresponds to absolute hypovolemia creating an imbalance between oxygen supply and consumption. This causes an impaired hemostasis, a systemic inflammatory response, and microvascular permeability which can lead to multiple organ failure (MOF). There is no specific treatment for the endothelial dysfunction that plays a major role in the evolution towards MOF. Mesenchymal stromal cells (MSC) have been used in clinical trials for their immunomodulation and tissue repair capabilities for many years. Moreover, we previously showed that IL-1β-primed-MSC (MSCp) attenuated HS-induced organ injuries. The objective of the study was to determine whether MSCp could prevent the onset of MOF after HS by preventing endothelial dysfunction.
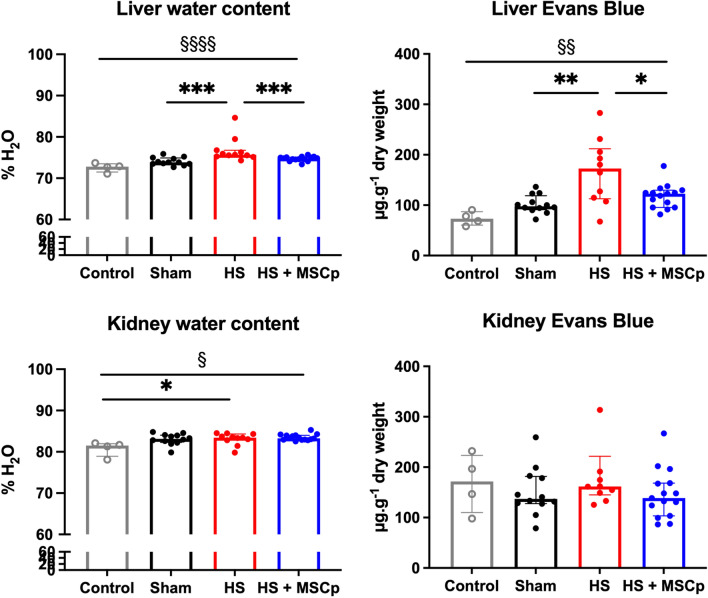
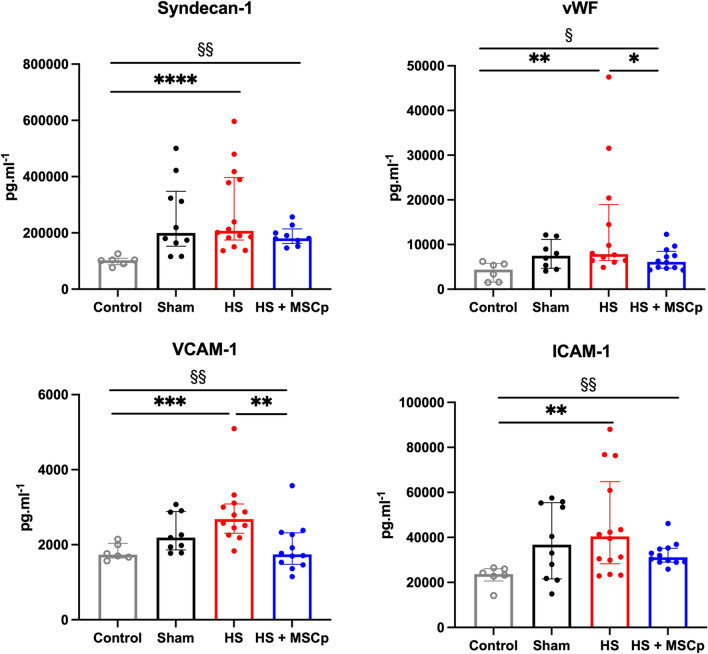
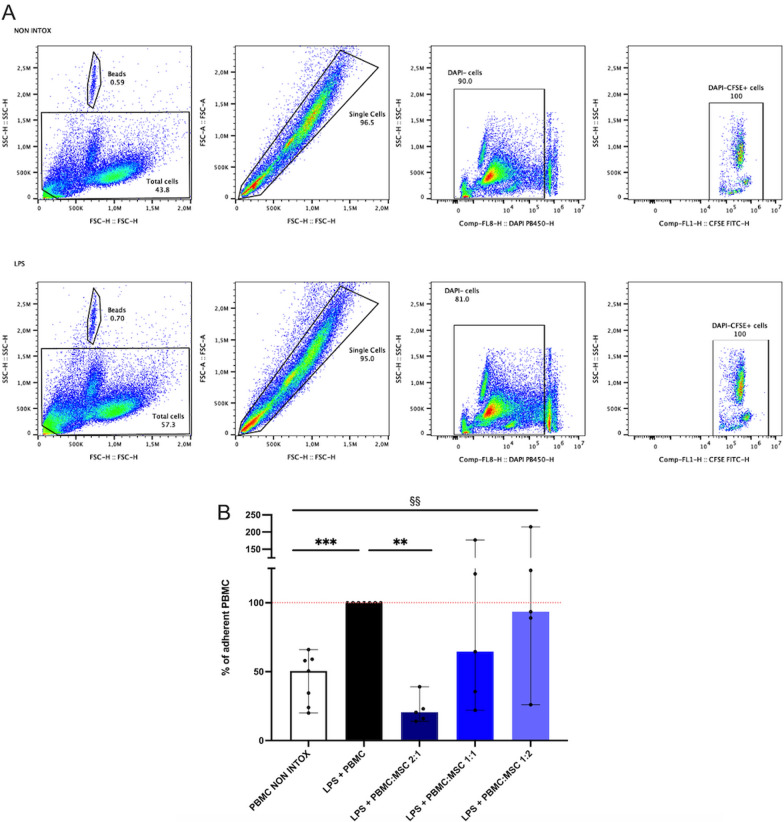
Methods: We established a rat model of HS, inducing 90 min of HS at a fixed mean arterial pressure of 35 mmHg, followed by resuscitation and transfusion. MSCp treatment was administered intravenously at the onset of resuscitation. After 6 h, we assessed plasma levels of endothelial markers, vascular permeability using Evans Blue (EB) dye, and renal and hepatic water content by measuring the wet-to-dry weight difference. Additionally, we investigated the ability of MSCp to inhibit leukocyte adhesion to activated endothelium in vitro.
Results: Our results indicate that early administration of MSCp significantly reduced the percentage of water content and EB dye in the liver but not in the kidney. These results were associated with a trend toward decreased plasma levels of Syndecan-1, ICAM-1, vWF, and VCAM-1. In vitro, MSCp reduced leukocyte-endothelial cell adhesion. Together, our results suggest that MSCp help to prevent endothelial dysfunction and vascular leakage, which, in turn, could protect the liver from injury.
Keywords: Hemorrhagic shock; Mesenchymal stromal cells; Multiple organ failure; Priming IL-1β; Vascular permeability.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All experimental procedures were performed in accordance with the European Community Council Directive (2010/63/UE) for the care and use of laboratory animals. Procedures on animals were authorized by the Ministère de l’Education Nationale, de l’Enseignement Supérieur et de la Recherche after approbation by the National Committee for Ethics in Animal. Experimentation (CEEALV/#9498). Consent for publication: Not applicable. Competing interests: The authors have no conflicts of interest to declare.
Figures

References
-
- Cannon JW. Hemorrhagic Shock. N Engl J Med. 2018;378:370–9. - PubMed
-
- Negoi I, Paun S, Hostiuc S, Stoica B, Tanase I, Negoi RI, et al. Mortality after acute trauma: Progressive decreasing rather than a trimodal distribution. J Acute Dis. 2015;4:205–9.
-
- Teixeira PGR, Inaba K, Hadjizacharia P, Brown C, Salim A, Rhee P, et al. Preventable or potentially preventable mortality at a mature trauma center. J Trauma. 2007;63:1338–46. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
