

Where are we with fractionation schedules and prescriptions in high-dose-rate 3D planning vaginal cuff brachytherapy?
- PMID: 39719951
- PMCID: PMC11664800
- DOI: 10.5114/jcb.2024.144183
Where are we with fractionation schedules and prescriptions in high-dose-rate 3D planning vaginal cuff brachytherapy?
Abstract
Purpose: Currently, there are many schedules for exclusive vaginal cuff brachytherapy (VCB). In 3D treatment planning for VCB dosimetry, parameters have not been analyzed. The aim of this study was to compare the most common schedules using dose-volume histogram metrics.
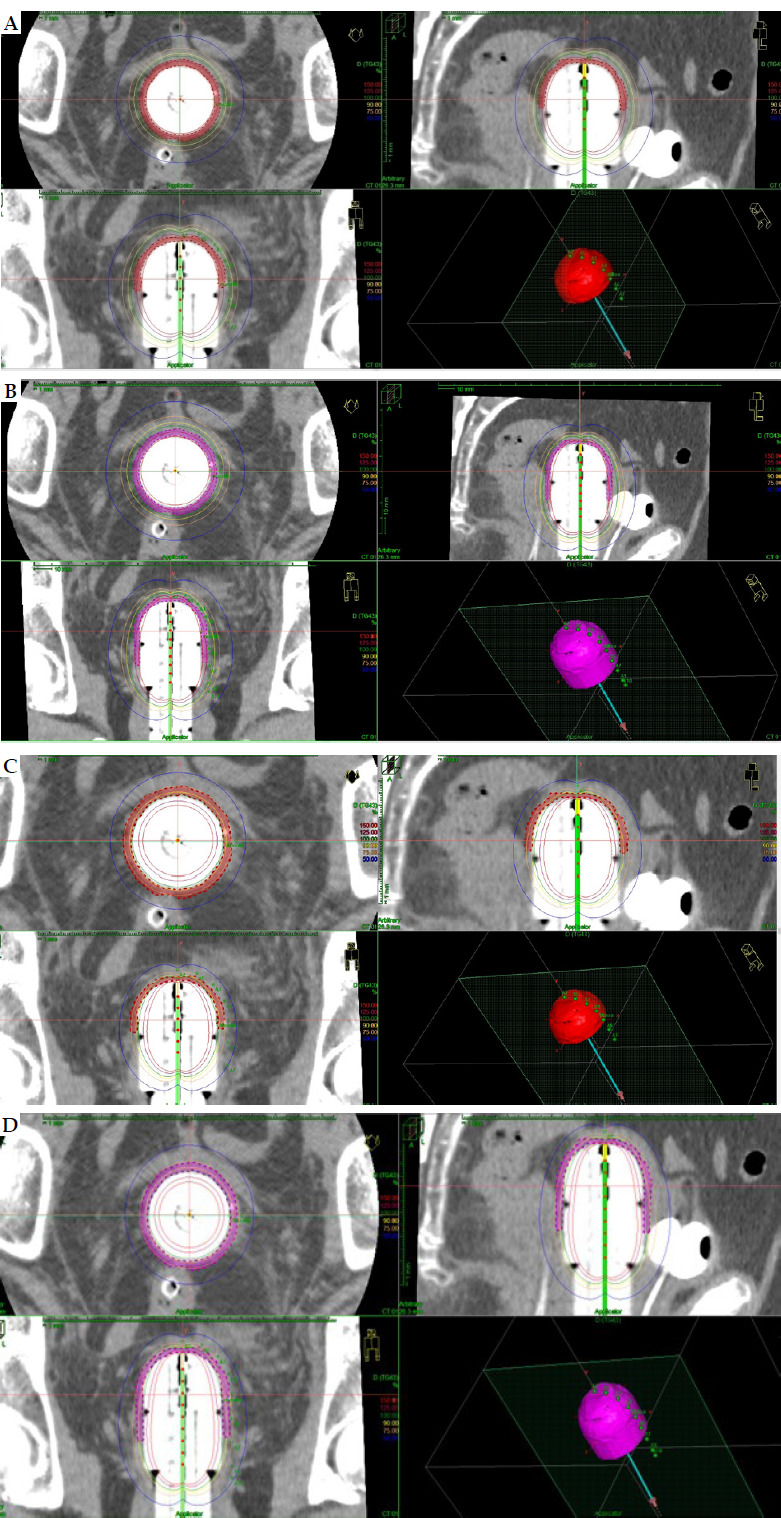
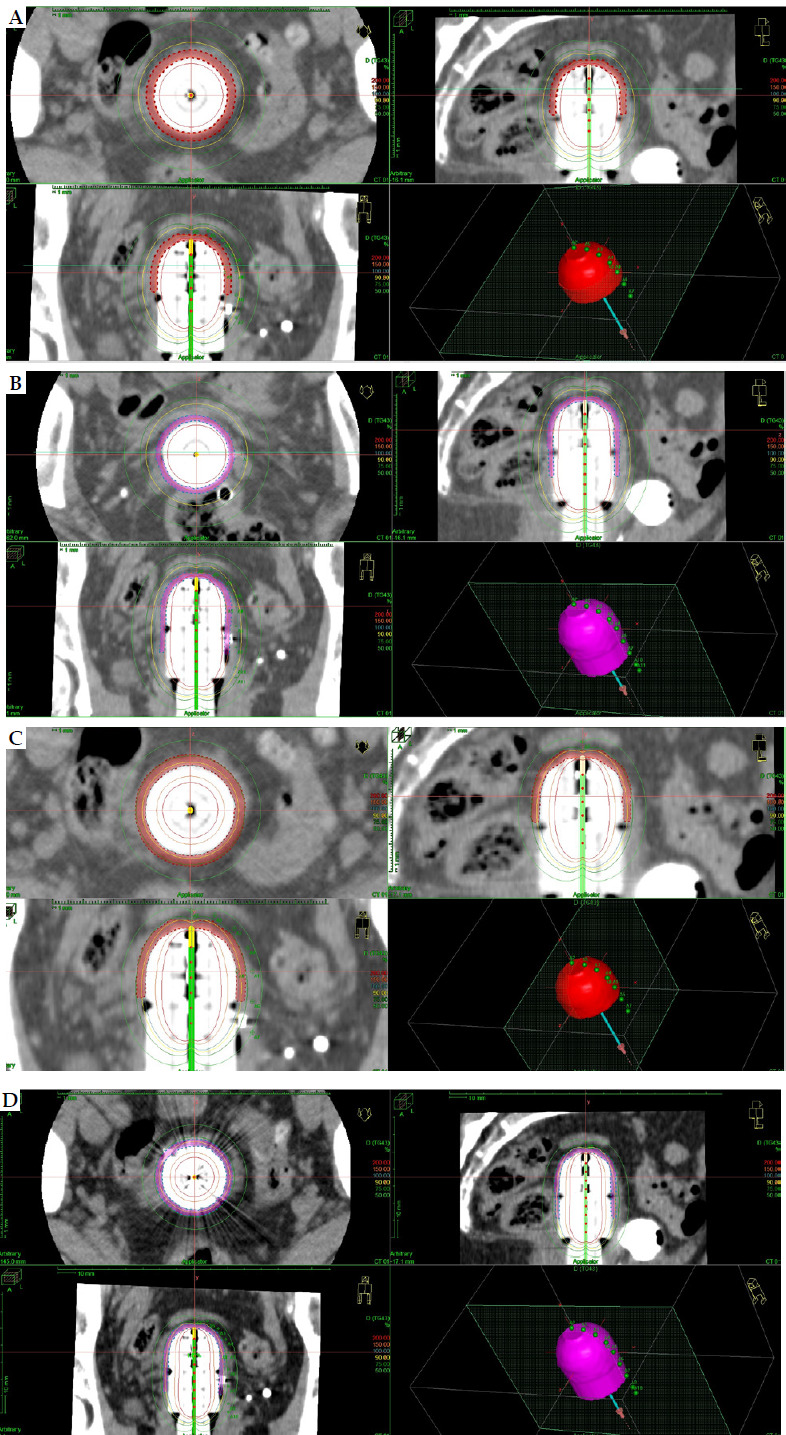
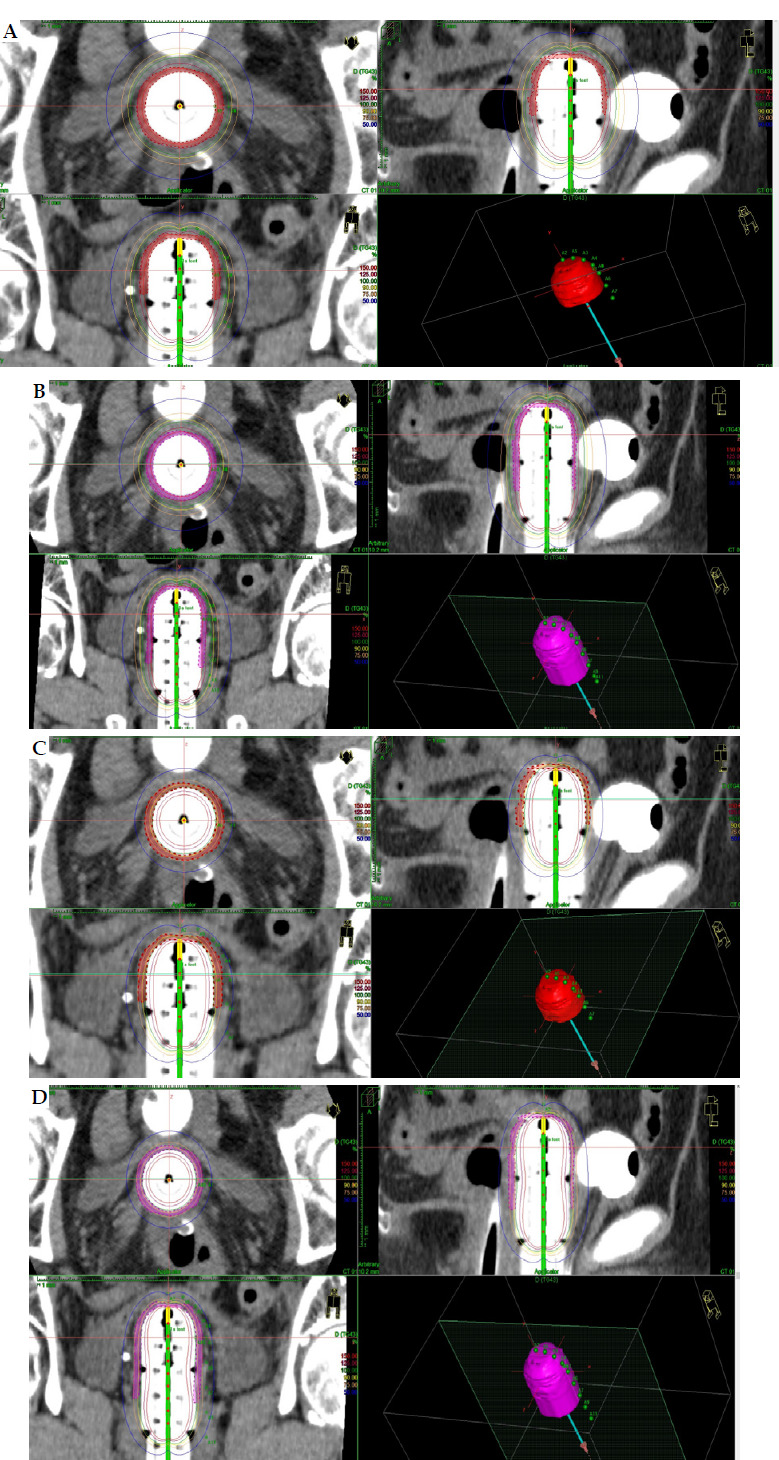
Material and methods: Three different computed tomography (CT) studies for vaginal cylinders of 3.5 cm, 3 cm, and 2.5 cm were performed. Clinical target volume (CTV) was delineated for 3 cm and 4 cm of vaginal length. Twelve schedules were analyzed obtaining overall vaginal surface dose (Gy) (EQD2 α/β = 10 and α/β = 3), overall D90 CTV (α/β = 10) (Gy), and overall D2cc (α/β = 3) for organs at risk (OARs), such as vagina, rectum, sigmoid, rectum, and bladder. Prescription at 5 mm from the applicator surface and at the surface were analyzed for each case.
Results: The overall vaginal surface dose and dose to CTV varied widely among the different schedules, and CTV delineation was necessary in case of surface prescription. The applicator diameter of 3.5 cm showed the best dosimetry results for vaginal surface dose. The overall D2cc OARs' doses changed in the different CT studies.
Conclusions: This dosimetry study allows for better selection of fractionation schedules, and helps to unify treatments among centers. Prospective studies are needed to establish the best schedule and CTV length in each patient using clinical data, such as late toxicity and relapses.
Keywords: endometrial cancer; schedules; vaginal-cuff brachytherapy.
Copyright © 2024 Termedia.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Similar articles
-
Are 7.5 Gy×2 fractions more efficient than 6 Gy×3 in exclusive postoperative endometrial cancer brachytherapy? A clinical and dosimetrical analysis.Radiother Oncol. 2023 Dec;189:109909. doi: 10.1016/j.radonc.2023.109909. Epub 2023 Sep 11. Radiother Oncol. 2023. PMID: 37699447
-
Dosimetric evaluation of different cylinder diameters in three-dimensional vaginal brachytherapy for early-stage endometrial cancer.J Cancer Res Clin Oncol. 2024 Nov 25;150(12):510. doi: 10.1007/s00432-024-05994-x. J Cancer Res Clin Oncol. 2024. PMID: 39585400 Free PMC article.
-
Rectal separation using hydroxypropyl methylcellulose in intracavitary brachytherapy of cervical cancer: an innovative approach.J Contemp Brachytherapy. 2016 Oct;8(5):399-403. doi: 10.5114/jcb.2016.62951. Epub 2016 Oct 11. J Contemp Brachytherapy. 2016. PMID: 27895681 Free PMC article.
-
Comparison of 2D vs. 3D dosimetry for Rotte 'Y' applicator high dose rate brachytherapy for medically inoperable endometrial cancer.Technol Cancer Res Treat. 2006 Oct;5(5):521-7. doi: 10.1177/153303460600500509. Technol Cancer Res Treat. 2006. PMID: 16981795
-
University Cooperation Platform (UCP) between Christian-Albrechts-University Kiel (Germany) and Chiang Mai University (Thailand): implementation of image-guided gynecological brachytherapy.J Contemp Brachytherapy. 2015 Feb;7(1):86-92. doi: 10.5114/jcb.2015.49444. Epub 2015 Mar 5. J Contemp Brachytherapy. 2015. PMID: 25829941 Free PMC article. Review.
References
-
- Harkenrider MM, Grover S, Erickson BAet al. . Vaginal brachytherapy for postoperative endometrial cancer: 2014 Survey of the American Brachytherapy. Brachytherapy 2016; 15: 23-29. - PubMed
-
- Hoskin P, Hellebust TP, Nout Ret al. . In: The GEC ESTRO Handbook of Brachytherapy. Second edition. Van Limbergen E, Pötter R, Hoskin P, Baltas D (Eds.). Part II: Clinical practice. ESTRO European Society for treatment Radiation and Oncology, Brussels: 2016.
-
- Wortman BG, Astreinidou E, Laman MSet al. . PORTEC Study Group Brachytherapy quality assurance in the PORTEC-4a trial for molecular-integrated risk profile guided adjuvant treatment of endometrial cancer. Radiother Oncol 2021; 155: 160-166. - PubMed
LinkOut - more resources
Full Text Sources