

The Toronto Tele-Retinal Screening Program for the Elderly in Long-Term Care: A Pilot Project
- PMID: 39720185
- PMCID: PMC11668048
- DOI: 10.2147/OPTH.S491154
The Toronto Tele-Retinal Screening Program for the Elderly in Long-Term Care: A Pilot Project
Abstract
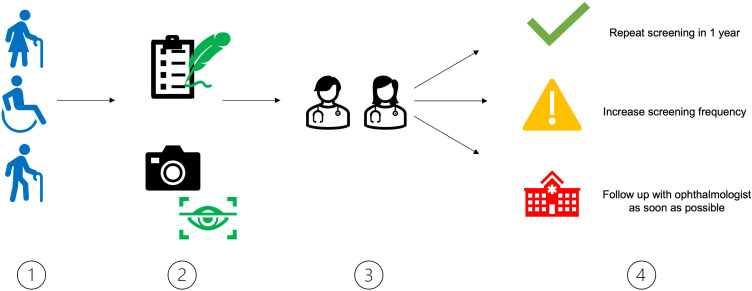
Objective: To report the results and feasibility of a pilot expansion of the Toronto Tele-Retinal Screening Program in an elderly long-term care home.
Methods: Long term care patients with Type II diabetes mellitus (DM) were screened between April 1, 2022, and July 1, 2022. Demographic and health data were collected through surveys.
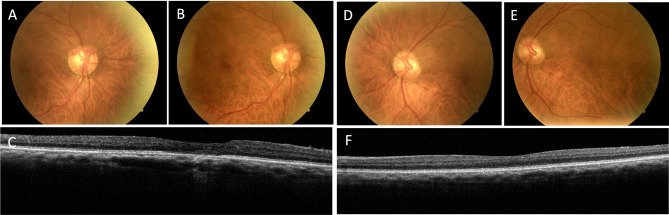
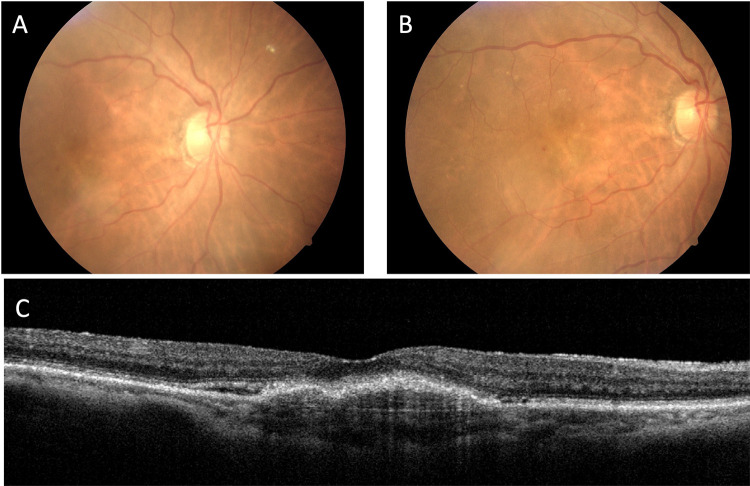
Results: A total of 28 patients were screened, with 85.7% successfully undergoing retinal imaging. Among imaged patients, 8.3% (2/24) required urgent follow-up. Pathologies identified included uncontrolled glaucoma (4.1%, 1/24), non-proliferative diabetic retinopathy (8.3%, 2/24), and age-related macular degeneration (45.8%, 11/24). The handheld camera successfully screened 60% (3/5) of patients with mobility issues. Overall, 90% (17/19) of patients rated their experience as either "brilliant" or "really good".
Discussion: This pilot project demonstrated the necessity for routine eye care in the elderly and the potential for widespread implementation of teleophthalmology in long-term care facilities. With only 14.3% (4/28) of patients unable to be imaged, this program offers a feasible, patient-friendly alternative to in-clinic screening. Future policies and practices in teleophthalmology should consider the unique needs of long-term care residents and the potential for reducing healthcare disparities through such a program.
Keywords: diabetes; elderly care; healthcare accessibility; retinopathy; telemedicine; teleophthalmology.
© 2024 Lim et al.
Conflict of interest statement
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by Diabetes Action Canada. This paper has been uploaded to JMIR Publications as a preprint:https://preprints.jmir.org/preprint/49188. The Authors declare that there is no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
