

Surgical interventions for spontaneous supratentorial intracerebral haemorrhage: a systematic review and network meta-analysis
- PMID: 39720609
- PMCID: PMC11667076
- DOI: 10.1016/j.eclinm.2024.102999
Surgical interventions for spontaneous supratentorial intracerebral haemorrhage: a systematic review and network meta-analysis
Abstract
Background: Surgical interventions for spontaneous supratentorial intracerebral haemorrhage (ICH) include conventional craniotomy (CC), decompressive craniectomy (DC), and minimally invasive surgery (MIS), with the latter encompassing endoscopic surgery (ES) and minimally invasive puncture surgery (MIPS). However, the superiority of surgery over conservative medical treatment (CMT) and the comparative benefits of different surgical procedures remain unclear. We aimed to evaluate the efficacy and safety of various surgical interventions for treating ICH.
Methods: In this systematic review and network meta-analysis, we searched PubMed, Cochrane Central Register of Controlled Trials, Embase, and ClinicalTrials.gov from inception to June 16, 2024. Eligible studies were randomised controlled trials (RCTs) comparing surgery (i.e., CC, ES, MIPS, or DC) with CMT or comparing different types of surgeries in patients with spontaneous supratentorial ICH. Paired reviewers independently screened citations, assessed the risk of bias of included trials, and extracted data. Primary outcomes were good functional outcome and mortality at 6 months. Secondary outcomes were good functional outcome and mortality at different follow-up times, complications (rebleeding, brain infection, pulmonary infection), and hematoma evacuation rate. The frequentist pairwise and network meta-analysis (NMA) were performed. The GRADE approach was used to evaluate the certainty of evidence. This study is registered with PROSPERO, CRD42024518961.
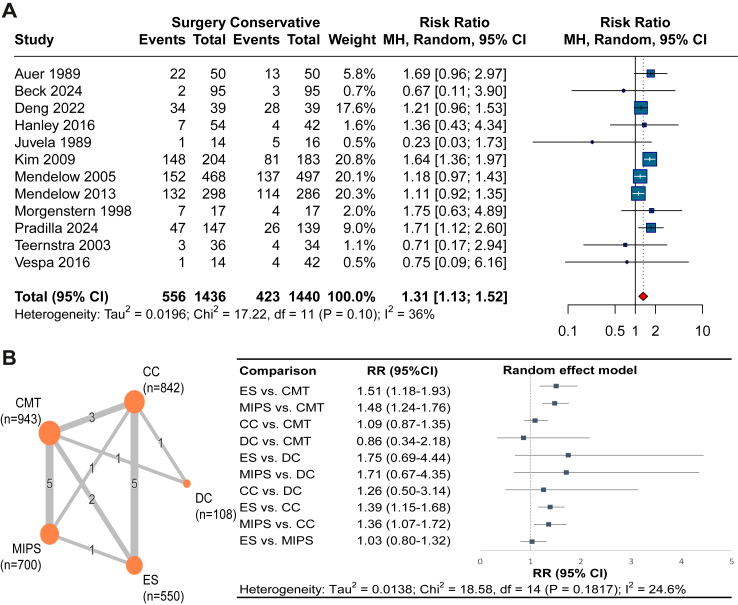
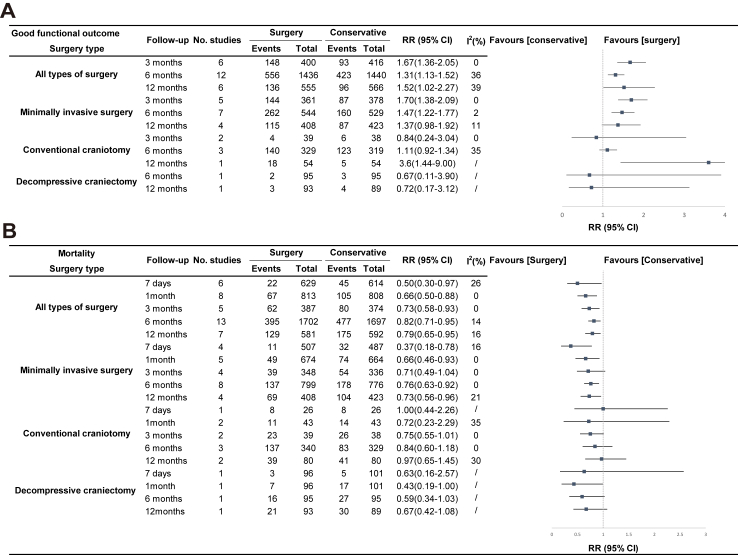
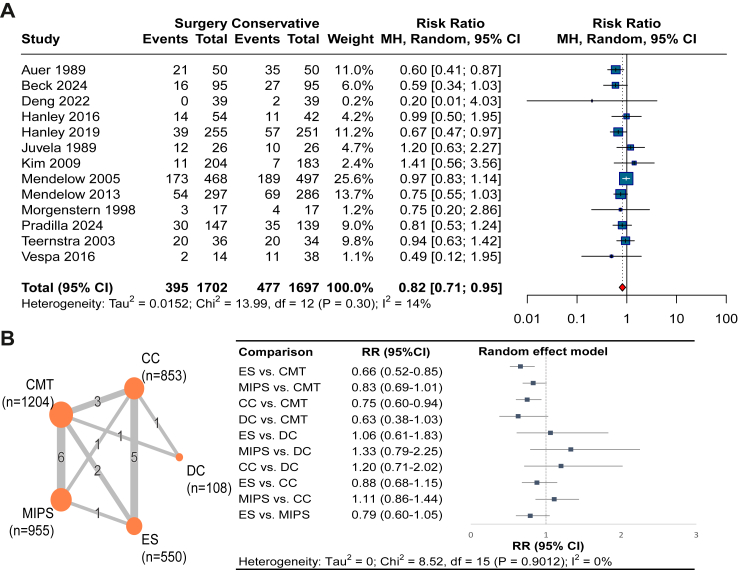
Findings: Of the 8573 total records identified by our searches, 31 studies (6448 patients) were eligible for the systematic review and network analysis. Compared with CMT, moderate certainty evidence showed that surgery improved good functional outcome (risk ratio [RR] 1.31, 95% CI 1.13-1.52; risk difference [RD] 9.1%, 95% CI 3.8 to 15.3; I 2 = 36%) and reduced mortality (RR 0.82, 95% CI 0.71-0.95; RD -5.1%, 95% CI -8.2 to -1.4; I 2 = 14%). Moderate certainty evidence from NMA suggested that compared with CMT, both ES (RR 1.51, 95% CI 1.18-1.93; RD 9.4%, 95% CI 3.3-17.1) and MIPS (RR 1.48, 95% CI 1.24-1.76; RD 15.7%, 95% CI 7.9-24.9) improved good functional outcome at 6 months, and both ES (RR 0.66, 95% CI 0.52-0.85; RD -17.0%, 95% CI -24.0 to -7.5) and CC (RR 0.75, 95% CI 0.60-0.94; RD -6.3%, 95% CI -10.1 to -1.5) reduced mortality at 6 months, whereas MIPS and DC showed a trend, although not statistically significant, towards a reduction in mortality. ES and MIPS also reduced pulmonary infection risk (ES RR 0.39, 95% CI 0.23-0.69; MIPS RR 0.35, 95% CI 0.20-0.60; RD -5.3%, 95% CI -6.6 to -3.3). ES showed higher hematoma evacuation than CC (MD: 7.03, 95% CI: 3.42-10.65; I 2 = 94%). No difference in rebleeding or brain infection was found between CC and MIS.
Interpretation: Current moderate certainty evidence suggested that surgical intervention of spontaneous supratentorial ICH, may be associated with improved functional outcomes and a reduced risk of death at 6 months. The advantages of surgical haematoma removal are particularly pronounced when MIS including ES and MIPS are employed. ES could improve functional outcomes, reduce the risk of mortality and pulmonary infection, and have a high hematoma evacuation rate, suggesting that it might be an optimal surgical treatment.
Funding: National Natural Science Foundation of China, National Science Fund for Distinguished Young Scholars, Fundamental Research Funds for the Central Public Welfare Research Institutes, and 1·3·5 project for disciplines of excellence, West China Hospital, Sichuan University.
Keywords: Intracerebral haemorrhage; Network meta-analysis; Surgical intervention; Systematic review.
© 2024 The Author(s).
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures


References
-
- Tsao C.W., Aday A.W., Almarzooq Z.I., et al. Heart disease and stroke statistics—2022 update: a report from the American heart association. Circulation. 2022;145:e153–e639. - PubMed
-
- Poon M.T.C., Fonville A.F., Al-Shahi Salman R. Long-term prognosis after intracerebral haemorrhage: systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. 2014;85:660–667. - PubMed
-
- Van Asch C.J., Luitse M.J., Rinkel G.J., Van Der Tweel I., Algra A., Klijn C.J. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9:167–176. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
