

Improving Procedural Pain Management for Newborns in a Level 3 Neonatal Intensive Care Unit: A Quality Improvement Initiative
- PMID: 39723316
- PMCID: PMC11669391
- DOI: 10.7759/cureus.74410
Improving Procedural Pain Management for Newborns in a Level 3 Neonatal Intensive Care Unit: A Quality Improvement Initiative
Abstract
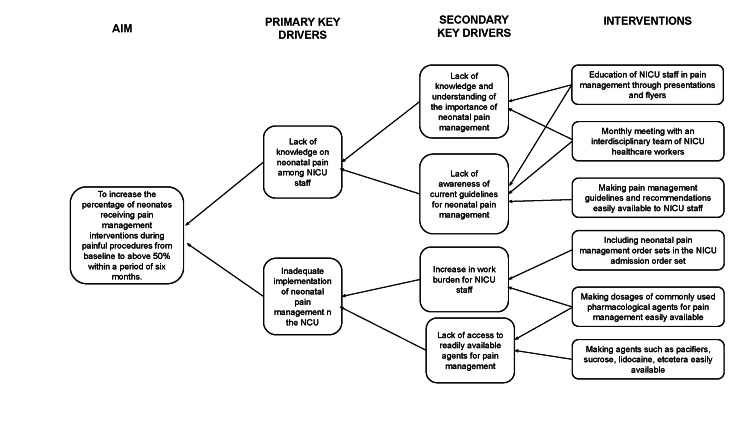
Introduction: Neonatal pain has been associated with numerous adverse outcomes, making pain management essential in the neonatal intensive care unit (NICU). Our specific, measurable, actionable, realistic, and timely (SMART) aim was to increase the proportion of neonates receiving pain management interventions during painful procedures from a baseline of less than 30% to above 50% within six months.
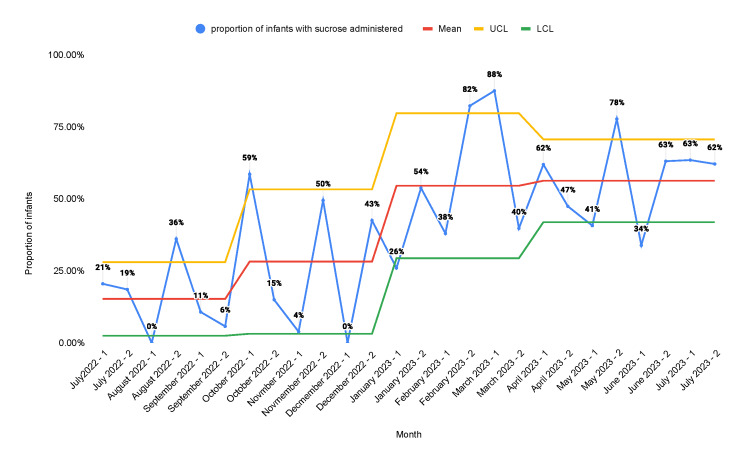
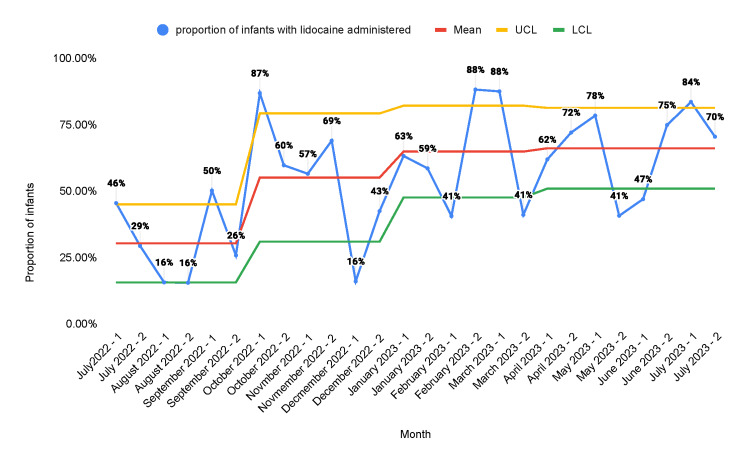
Methods: The Plan-Do-Study-Act (PDSA) model for improvement methodology was employed to improve pain management in the NICU between August 2022 and July 2023. Interventions included educational campaigns, monthly meetings, weekly huddles, smart order sets, readily available medication information, and accessibility. Data was collected by reviewing the electronic health record (EHR), and survey data was collected through anonymous surveys of the NICU staff. The outcome measures were the proportion of sucrose and 4% lidocaine orders placed and the proportion of procedures that received pain management interventions.
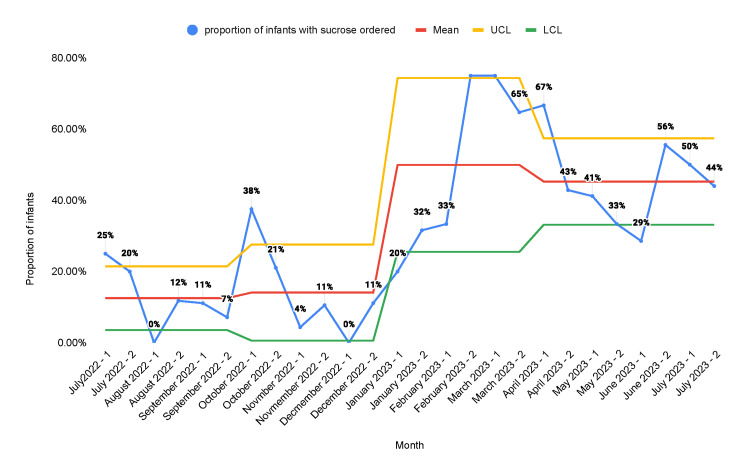
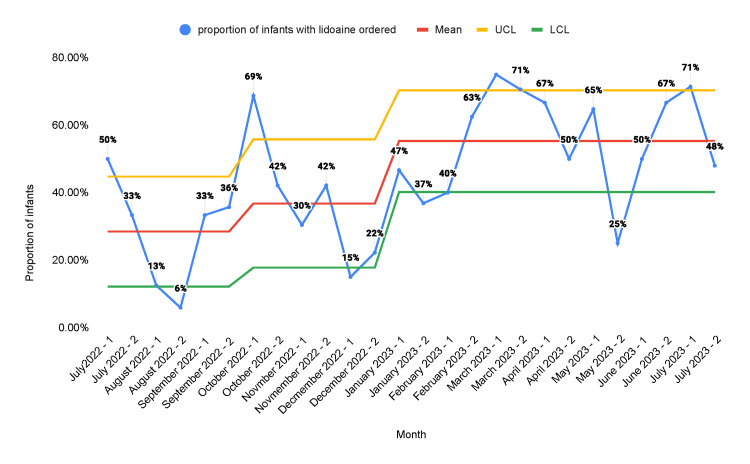
Results: During the period from August 2022 to July 2023, there were 383 newborns admitted to the NICU. On average, each newborn underwent 42.8 procedures during their hospital stay. The proportion of neonates who were ordered sucrose and 4% lidocaine increased from a baseline of 7% and 21% to 43% and 54% after the second PDSA cycle, respectively. The proportion of procedures for which sucrose and lidocaine were administered increased from 16% and 21% at baseline to 54% and 65% after the second PDSA cycle.
Conclusion: The quality improvement (QI) methodology in conjunction with the education of NICU staff and the incorporation of smart order sets can be used to effectively increase the use of pain management interventions in the NICU.
Keywords: neonates; oral sucrose; pain; pdsa model; quality improvement.
Copyright © 2024, Sriraman et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Institutional Review Board (IRB) at the State University of New York (SUNY) Downstate Medical Center issued approval 1952090-1. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Epidemiology of painful procedures performed in neonates: a systematic review of observational studies. Cruz MD, Fernandes AM, Oliveira CR. Eur J Pain. 2016;20:489–498. - PubMed
-
- The neurobiology of pain: developmental aspects. Fitzgerald M, Beggs S. Neuroscientist. 2001;7:246–257. - PubMed
-
- Pathway to pain. Farley S. Nat Rev Neurosci. 2003;4:158.
-
- Treatment of pain and stress in the neonate: when and how. Khurana S, Whit Hall R, Anand KJ. Neoreviews. 2005;6:0–86.
LinkOut - more resources
Full Text Sources