

Effect of an intensive lifestyle intervention on cystatin C-based kidney function in adults with overweight and obesity: From the PREDIMED-Plus trial
- PMID: 39723807
- PMCID: PMC11771574
- DOI: 10.1111/joim.20038
Effect of an intensive lifestyle intervention on cystatin C-based kidney function in adults with overweight and obesity: From the PREDIMED-Plus trial
Abstract
Background: Large-scale trials evaluating a multicomponent lifestyle intervention aimed at weight loss on kidney function are lacking.
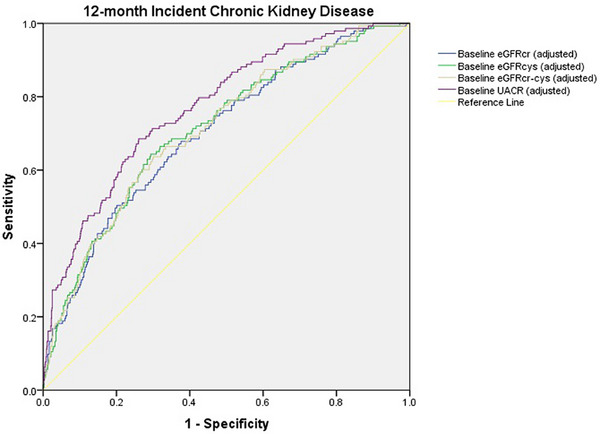
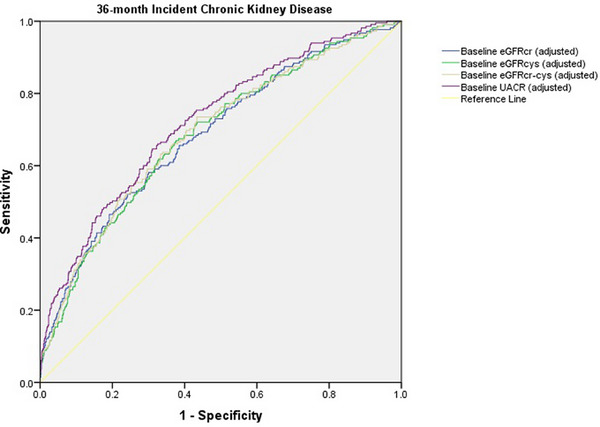
Methods: This was a post hoc analysis of the "PREvención con DIeta MEDiterránea-Plus" (PREDIMED-Plus) randomized controlled trial, including patients with overweight/obesity and metabolic syndrome, measured cystatin C and creatinine. Participants were randomly assigned (1:1) to an intensive weight loss lifestyle intervention (intervention group [IG]) consisting of an energy-restricted Mediterranean diet (MedDiet), physical activity promotion and behavioral support, or a control group (CG) receiving ad libitum MedDiet recommendations. The primary outcome was between-group differences in cystatin C-based kidney function (cystatin C-based estimated glomerular filtration rate-eGFRcys-and combined cystatin C-creatinine-based eGFR-eGFRcr-cys) change from baseline to 12 and 36 months. Secondary outcomes included between-group differences in creatinine-based eGFR (eGFRcr) and urinary albumin-to-creatinine ratio (UACR) change and the predictive capacity of these formulas at baseline for new-onset chronic kidney disease (CKD).
Results: A total of 1909 participants (65 ± 5 years, 54% men) were included. Twelve-month decline in eGFRcys, eGFRcr-cys, and eGFRcr was greater in the CG compared to the IG, with between-group differences of -1.77 mL/min/1.73 m2 [95% confidence interval -2.92 to -0.63], -1.37 [-2.22 to -0.53], and -0.91 [-1.74 to -0.71], respectively. At 36 months, the decline in eGFRcr-cys and eGFRcr was greater in the CG. No between-group differences in UACR were found. Significant adjusted areas under the curve for baseline eGFRcys and eGFRcr-cys were observed for incident CKD at 36 months, which were similar to those for eGFRcr and UACR.
Conclusions: In older adults with overweight/obesity and metabolic syndrome, the PREDIMED-Plus intervention may be an optimal approach to preserve kidney function.
Keywords: Mediterranean diet; cystatin C; kidney function; lifestyle intervention; obesity.
© 2025 The Author(s). Journal of Internal Medicine published by John Wiley & Sons Ltd on behalf of Association for Publication of The Journal of Internal Medicine.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- CM 17/00169/Rio Hortega
- CM22/00217/Rio Hortega
- 19/00054/Juan Rodes JR
- Fondo Europeo de Desarrollo Regional-FEDER
- LIKIDI study OBN20PI01/2020/CIBER Fisiopatología de la Obesidad y Nutrición (CIBEROBN)
- PI13/00673/European Regional Development Fund
- PI13/00492/European Regional Development Fund
- PI13/00272/European Regional Development Fund
- PI13/01123/European Regional Development Fund
- PI13/00462/European Regional Development Fund
- PI13/00233/European Regional Development Fund
- PI13/02184/European Regional Development Fund
- PI13/00728/European Regional Development Fund
- PI13/01090/European Regional Development Fund
- PI13/01056/European Regional Development Fund
- PI14/01722/European Regional Development Fund
- PI14/00636/European Regional Development Fund
- PI14/00618/European Regional Development Fund
- PI14/00696/European Regional Development Fund
- PI14/01206/European Regional Development Fund
- PI14/01919/European Regional Development Fund
- PI14/00853/European Regional Development Fund
- PI14/01374/European Regional Development Fund
- PI14/00972/European Regional Development Fund
- PI14/00728/European Regional Development Fund
- PI14/01471/European Regional Development Fund
- PI16/00473/European Regional Development Fund
- PI16/00662/European Regional Development Fund
- PI16/01873/European Regional Development Fund
- PI16/01094/European Regional Development Fund
- PI16/00501/European Regional Development Fund
- PI16/00533/European Regional Development Fund
- PI16/00381/European Regional Development Fund
- PI16/00366/European Regional Development Fund
- PI16/01522/European Regional Development Fund
- PI16/01120/European Regional Development Fund
- PI17/00764/European Regional Development Fund
- PI17/01183/European Regional Development Fund
- PI17/00855/European Regional Development Fund
- PI17/01347/European Regional Development Fund
- PI17/00525/European Regional Development Fund
- PI17/01827/European Regional Development Fund
- PI17/00532/European Regional Development Fund
- PI17/00215/European Regional Development Fund
- PI17/01441/European Regional Development Fund
- PI17/00508/European Regional Development Fund
- PI17/01732/European Regional Development Fund
- PI17/00926/European Regional Development Fund
- PI19/00957/European Regional Development Fund
- PI19/00386/European Regional Development Fund
- PI19/00309/European Regional Development Fund
- PI19/01032/European Regional Development Fund
- PI19/00576/European Regional Development Fund
- PI19/00017/European Regional Development Fund
- PI19/01226/European Regional Development Fund
- PI19/00781/European Regional Development Fund
- PI19/01560/European Regional Development Fund
- PI19/01332/European Regional Development Fund
- PI20/01802/European Regional Development Fund
- PI20/00138/European Regional Development Fund
- PI20/01532/European Regional Development Fund
- PI20/00456/European Regional Development Fund
- PI20/00339/European Regional Development Fund
- PI20/00557/European Regional Development Fund
- PI20/00886/European Regional Development Fund
- PI20/01158/European Regional Development Fund
- CM 17/00169/Instituto de Salud Carlos III
- JR 19/00054/Instituto de Salud Carlos III
- CM22/00217/Instituto de Salud Carlos III
- PI20/01802/Instituto de Salud Carlos III
- PI20/00138/Instituto de Salud Carlos III
- PI20/01532/Instituto de Salud Carlos III
- PI20/00456/Instituto de Salud Carlos III
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
