

Ultrasound-guided Percutaneous Cryoneurolysis for the Treatment of Pain after Traumatic Rib Fracture: A Randomized, Active-controlled, Participant- and Observer-masked Study
- PMID: 39723886
- PMCID: PMC11801435
- DOI: 10.1097/ALN.0000000000005328
Ultrasound-guided Percutaneous Cryoneurolysis for the Treatment of Pain after Traumatic Rib Fracture: A Randomized, Active-controlled, Participant- and Observer-masked Study
Abstract
Background: Traumatic rib fractures are associated with pain lasting weeks to months and a decreased ability to inspire deeply or cough to clear secretions. Ultrasound-guided percutaneous cryoneurolysis involves reversibly ablating peripheral nerve(s) using exceptionally low temperature with a transdermal probe, resulting in a prolonged nerve block with a duration measured in months. The authors hypothesized that cryoneurolysis would improve analgesia and inspired volume after rib fracture.
Methods: Adults with one to six traumatic rib fractures were randomized to either active cryoneurolysis and sham peripheral nerve block or sham cryoneurolysis and active peripheral nerve block in a participant/observer-masked fashion. The primary endpoint was the maximum inspired volume the day after the procedure as measured with an incentive spirometer.
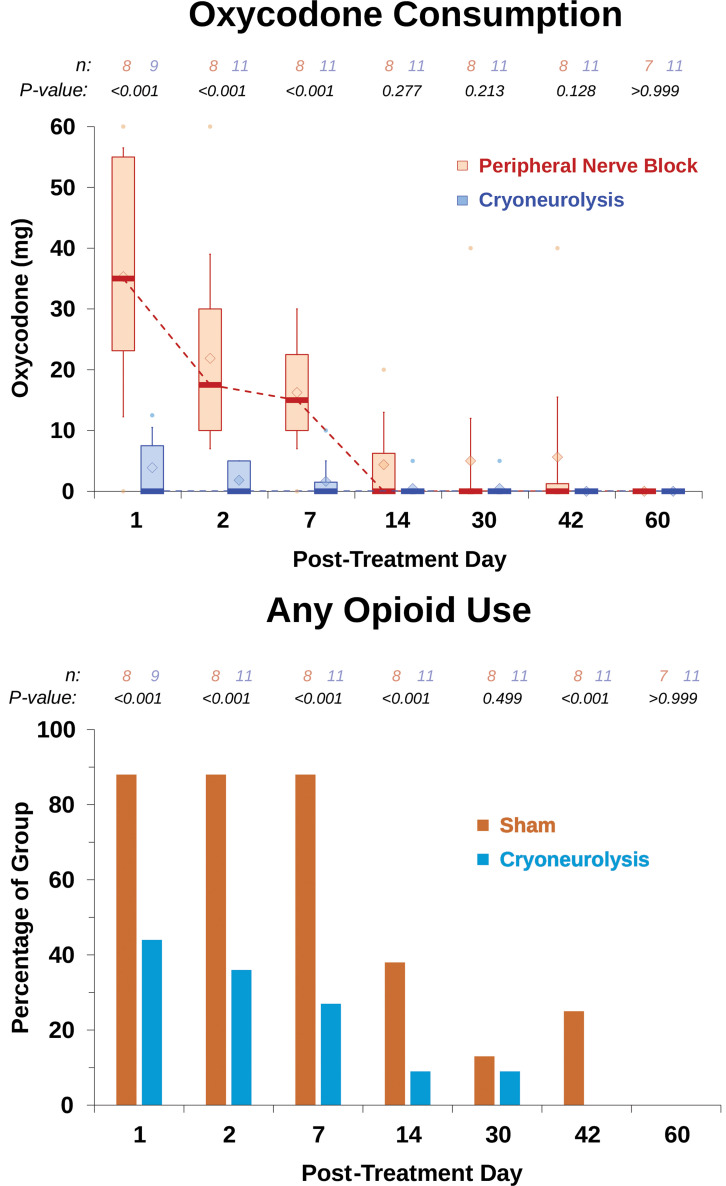
Results: The day after the procedure, the unadjusted median [interquartile range] maximum inspired volume for participants who received cryoneurolysis (n = 11) was 2,250 ml [1,500, 2,500 ml] versus 1,300 ml [750, 2,500 ml] for peripheral nerve block (n = 9, mean difference, 496; 95% CI, -428 to 1,420; t test P = 0.269). When adjusted for covariates ( e.g. , baseline lung volume), the cryoneurolysis group had an estimated 793 ml greater mean volume than peripheral nerve block (95% CI, 273 to 1,312 ml; analysis of covariance P = 0.005). Improvement from baseline in maximum inspired volume for cryoneurolysis was 1,000 ml [1,000, 1,375 ml] versus 300 ml [0, 1,000 ml] for peripheral nerve block ( t test P = 0.002). This was equivalent to an improvement over baseline of 100% [90%, 188%] for cryoneurolysis versus 30% [0%, 50%] for peripheral nerve block ( t test P = 0.003). Average daily pain scores were generally lower for the cryoneurolysis group throughout the first month. Total cumulative oxycodone equivalents were 5 mg [0, 13 mg] for cryoneurolysis versus 45 mg [43, 135 mg] for peripheral nerve block ( t test P = 0.013).
Conclusions: Ultrasound-guided percutaneous cryoneurolysis improves maximum inspired lung volume while concurrently decreasing pain and opioid consumption after traumatic rib fracture. These results should be considered preliminary, requiring confirmation with a trial including a larger sample size.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc., on behalf of the American Society of Anesthesiologists.
Conflict of interest statement
Drs. Finneran and Ilfeld’s institution has received funding and/or product from Epimed International (Dallas, Texas) for other research studies, SPR Therapeutics (Cleveland, Ohio), Infutronix (Natick, Massachusetts), Masimo (Irvine, California), Varian Medical Systems (Palo Alto, California), and Avanos Medical (Irvine, California). Dr. Trescot. has served on an advisory board for Atricure, (Mason, Ohio) and is the chief medical officer for Stimwave Technologies (Pompano, Florida). Dr. Donohue has served on scientific advisory boards for Biogen (Cambridge, Massachusetts), Eli Lilly (Indianapolis, Indiana), and Neurotrack Technologies (Redwood City, California) and has consulted for Roche. His spouse is a full-time employee of Janssen (Beerse, Belgium). Dr. Schaar’s institution has received funding and/or product from Epimed International and Infutronix for other research studies. The other authors declare no competing interests.
Figures





References
-
- Ziegler DW, Agarwal NN: The morbidity and mortality of rib fractures. J Trauma 1994; 37:975–9 - PubMed
-
- Martin TJ, Eltorai AS, Dunn R, et al. : Clinical management of rib fractures and methods for prevention of pulmonary complications: A review. Injury 2019; 50:1159–65 - PubMed
-
- Kerr-Valentic MA, Arthur M, Mullins RJ, Pearson TE, Mayberry JC: Rib fracture pain and disability: Can we do better? J Trauma 2003; 54:1058–63; discussion 1063 - PubMed
