

The role and potential of digital breast tomosynthesis in neoadjuvant systemic therapy evaluation for optimising breast cancer management: a pictorial essay
- PMID: 39724185
- PMCID: PMC11919077
- DOI: 10.1093/bjr/tqae252
The role and potential of digital breast tomosynthesis in neoadjuvant systemic therapy evaluation for optimising breast cancer management: a pictorial essay
Abstract
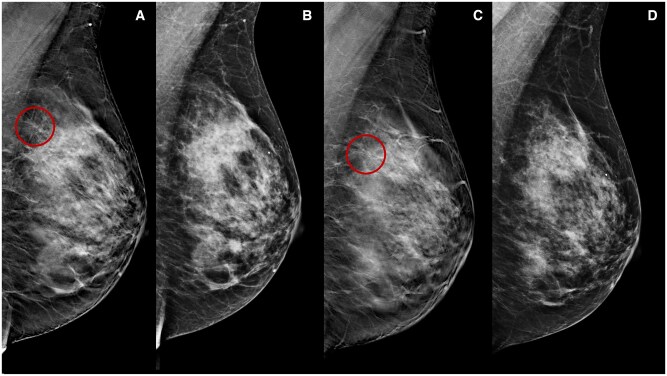
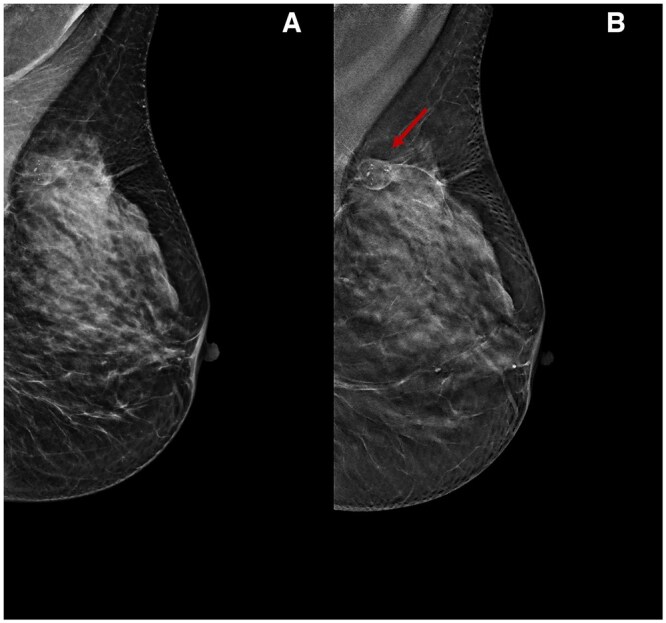
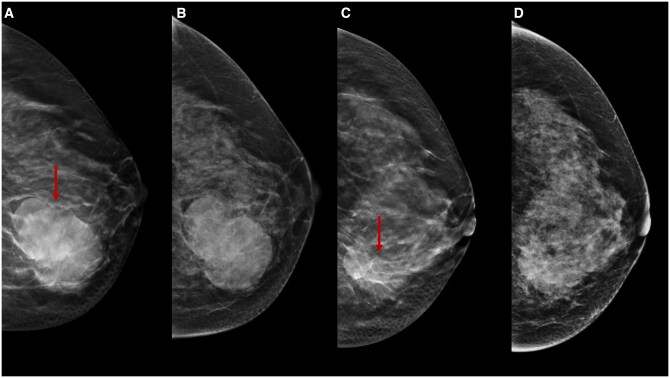
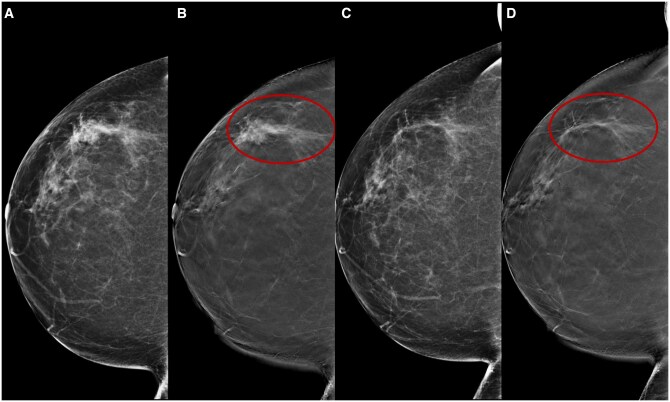
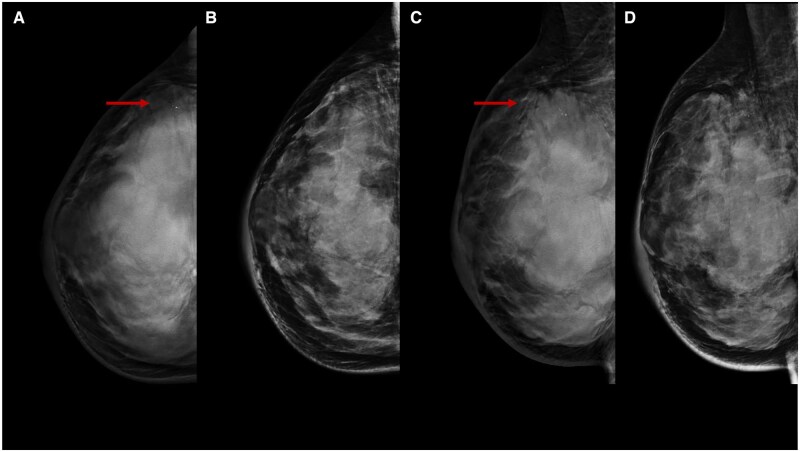
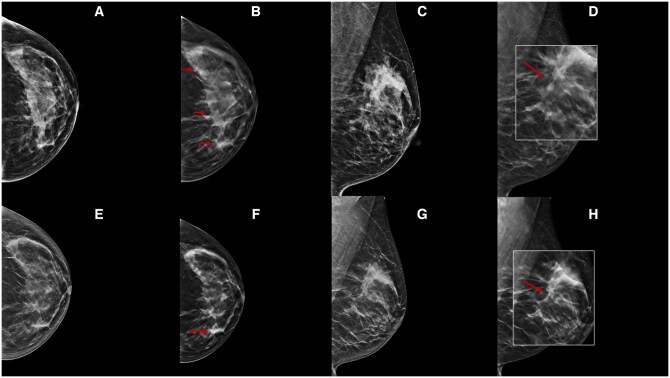
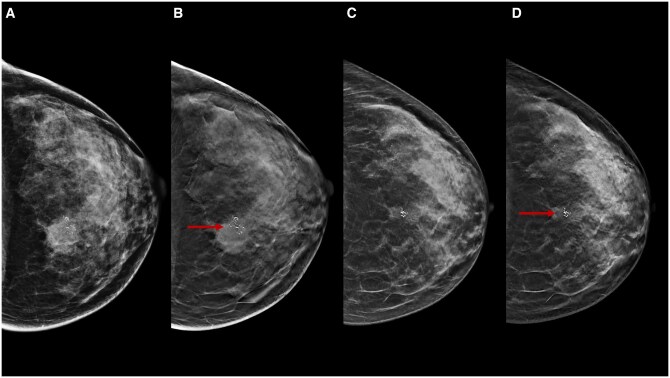
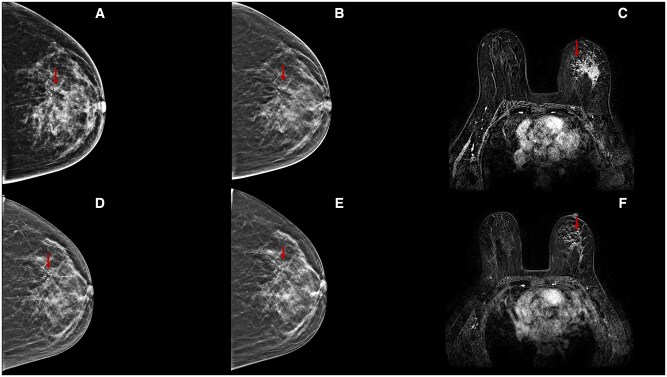
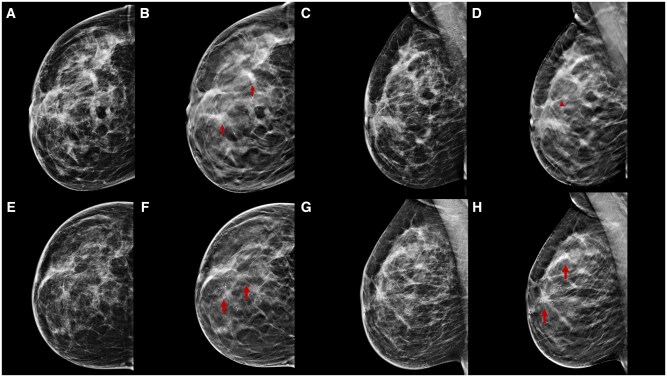
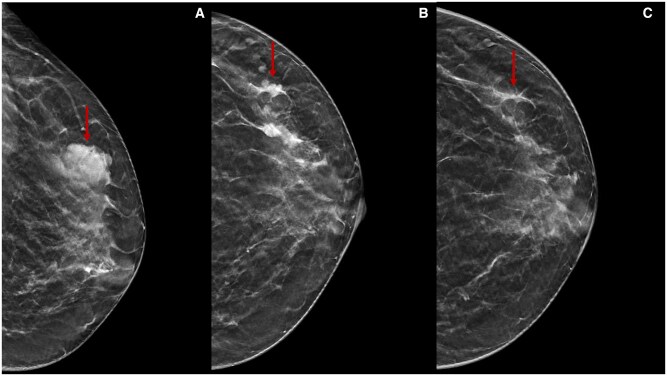
Neoadjuvant therapy (NT) has become the gold standard for treating locally advanced breast cancer (BC). The assessment of pathological response (pR) post-NT plays a crucial role in predicting long-term survival, with contrast-enhanced MRI currently recognised as the preferred imaging modality for its evaluation. Traditional imaging techniques, such as digital mammography (DM) and ultrasonography (US), encounter difficulties in post-NT assessments due to breast density, lesion changes, fibrosis, and molecular patterns. Digital breast tomosynthesis (DBT) offers solutions to prevalent challenges in DM, such as tissue overlap, and facilitates a comprehensive assessment of lesion morphology, dimensions, and margins. Studies suggest that DBT correlates more accurately with pathology than DM and US, showcasing its potential advantages. This pictorial essay demonstrates the potential of DBT as a complementary tool to DM for assessing pR after NT, including instances of true- and false-positive assessments correlated with histopathological findings. In conclusion, DBT emerges as a valuable adjunct to DM, effectively addressing its limitations in post-NT assessment. The technology's potential to diminish tissue overlap, improve discrimination, and provide multi-dimensional perspectives demonstrates promising results, indicating its utility in scenarios where MRI is contraindicated or inaccessible.
Keywords: breast cancer; neoadjuvant therapy; tomosynthesis.
© The Author(s) 2024. Published by Oxford University Press on behalf of the British Institute of Radiology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
[Comparison of the Diagnostic Values of Dynamic Enhanced Magnetic Resonance Imaging,Digital Breast Tomosynthesis,and Digital Mammography for Early Breast Cancer].Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2019 Oct 30;41(5):667-672. doi: 10.3881/j.issn.1000-503X.10938. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2019. PMID: 31699198 Chinese.
-
Utility of Breast MRI for Further Evaluation of Equivocal Findings on Digital Breast Tomosynthesis.AJR Am J Roentgenol. 2018 Nov;211(5):1171-1178. doi: 10.2214/AJR.17.18866. Epub 2018 Sep 12. AJR Am J Roentgenol. 2018. PMID: 30207789
-
Not all false positive diagnoses are equal: On the prognostic implications of false-positive diagnoses made in breast MRI versus in mammography / digital tomosynthesis screening.Breast Cancer Res. 2018 Feb 9;20(1):13. doi: 10.1186/s13058-018-0937-7. Breast Cancer Res. 2018. PMID: 29426360 Free PMC article.
-
Supplemental Screening as an Adjunct to Mammography for Breast Cancer Screening in People With Dense Breasts: A Health Technology Assessment.Ont Health Technol Assess Ser. 2023 Dec 19;23(9):1-293. eCollection 2023. Ont Health Technol Assess Ser. 2023. PMID: 39364436 Free PMC article.
-
Overview of the evidence on digital breast tomosynthesis in breast cancer detection.Breast. 2013 Apr;22(2):101-108. doi: 10.1016/j.breast.2013.01.017. Epub 2013 Feb 16. Breast. 2013. PMID: 23422255 Review.
Cited by
-
Overcoming Barriers for Breast Cancer Detection in Women with High Breast Density [Letter].Patient Prefer Adherence. 2025 Feb 15;19:359-360. doi: 10.2147/PPA.S518898. eCollection 2025. Patient Prefer Adherence. 2025. PMID: 39974668 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
