

Nomogram model for predicting secondary infection in critically ill patients with heatstroke: A pilot study from China
- PMID: 39724279
- PMCID: PMC11670984
- DOI: 10.1371/journal.pone.0316254
Nomogram model for predicting secondary infection in critically ill patients with heatstroke: A pilot study from China
Abstract
Objective: In this retrospective analysis, we explored the clinical characteristics and risk factors of secondary infections in patients with severe heatstroke with the aim to gain epidemiological insights and identify risk factors for secondary infections.
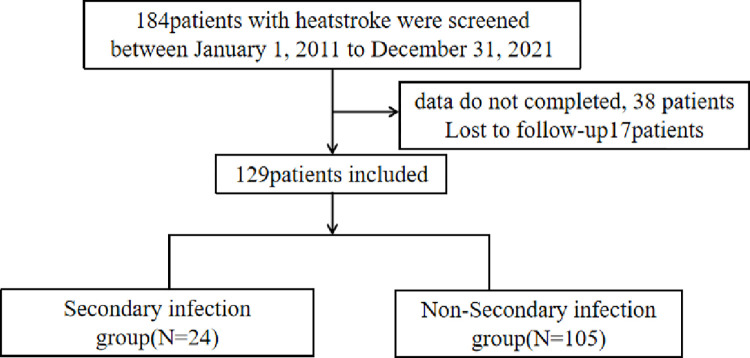
Method: The study included 129 patients with severe heatstroke admitted to the General Hospital of the Southern Theater Command of the PLA between January 1, 2011, and December 31, 2021. Patients were divided into an infection group (n = 24) and a non-infection group (n = 105) based on infection occurrence within 48 h of intensive care unit (ICU) admission. Clinical indicators, infection indicators, and clinical outcomes within 24 h of ICU admission were collected and compared between the groups. Independent risk factors for infection in patients with severe heatstroke were analyzed using univariate and multivariate analyses. A nomogram model was constructed, evaluated, and validated.
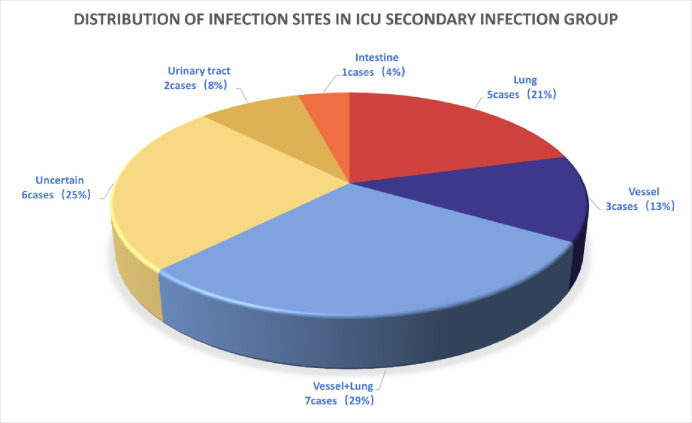
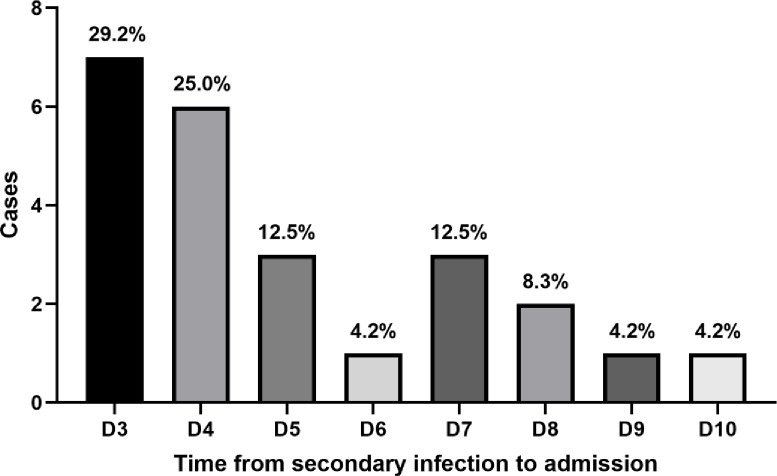
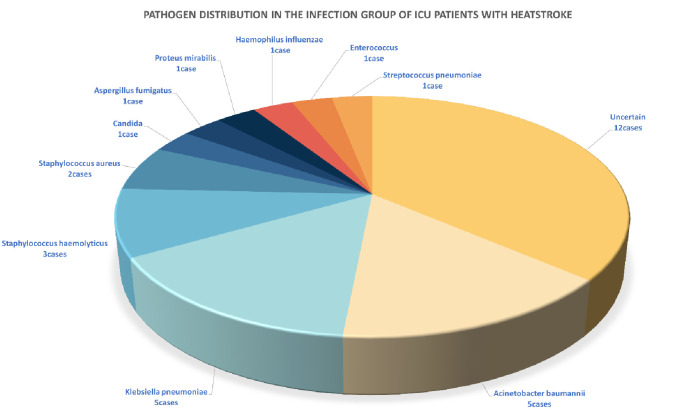
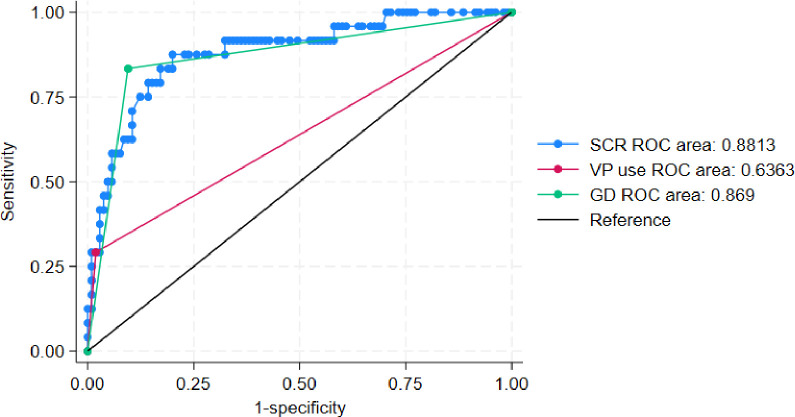
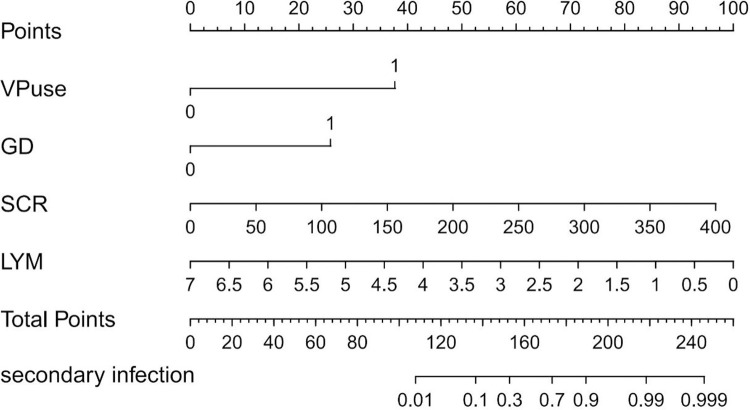
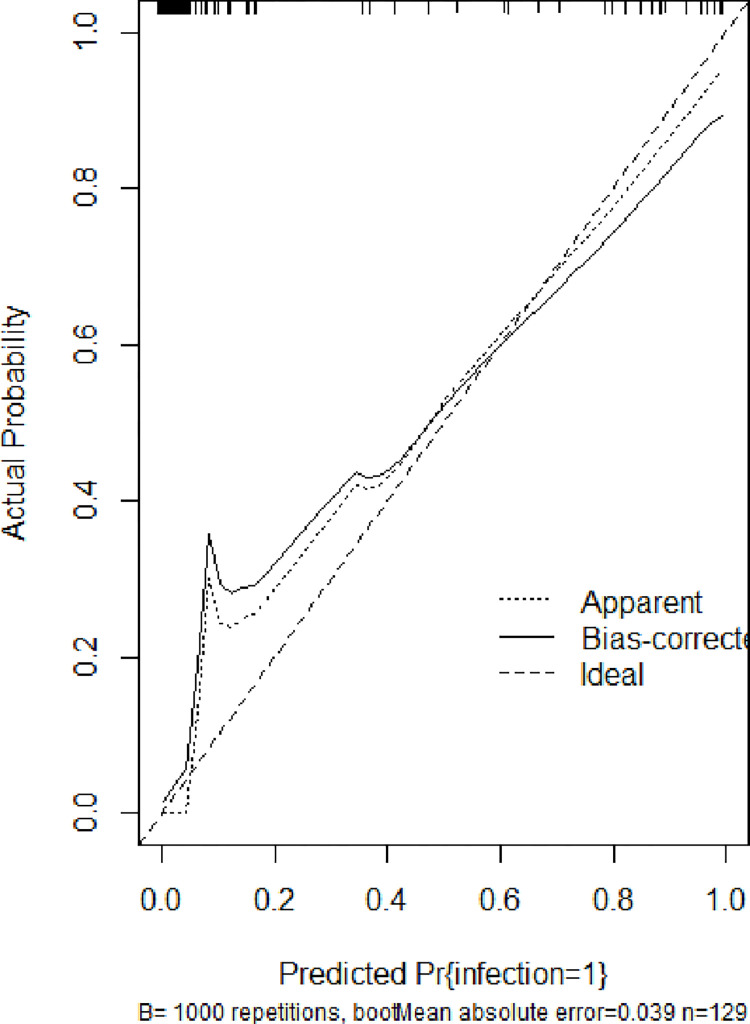
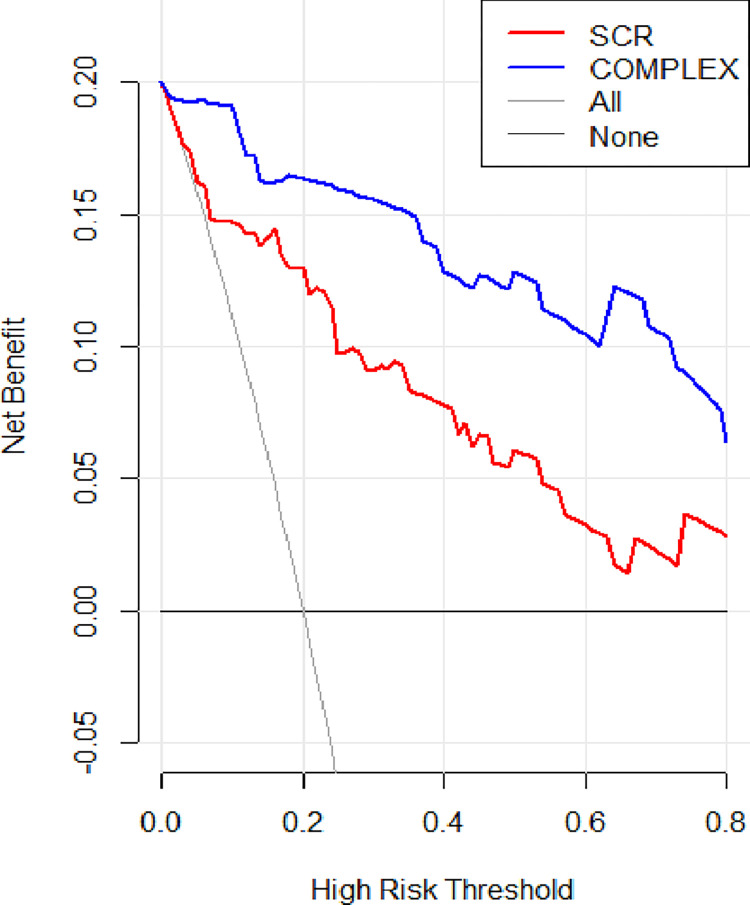
Result: Among the 129 patients with heatstroke, 24 developed secondary infections. Infections occurred between days 3 and 10 post-ICU admission, primarily affecting the lungs. Multivariate analysis identified vasopressor use, serum creatinine level, and gastrointestinal dysfunction at admission as independent risk factors, while elevated lymphocyte count (odds ratio [OR] = 0.167; 95% confidence interval [CI] 0.049-0.572; P = 0.004) was protective against severe heatstroke. Infected patients required longer durations of mechanical ventilation (OR = 2.764; 95% CI, 1.735-4.405; P = 0.044) and total hospital stay than those in the non-infection group. The nomogram model demonstrated clinical feasibility.
Conclusion: Increased lymphocyte count is an independent protective factor against infections in patients with severe heatstroke. Vasopressor use, gastrointestinal dysfunction, and elevated serum creatinine levels are independent risk factors. These indicators can aid clinicians in assessing infection risk in patients with severe heatstroke.
Copyright: © 2024 Lin et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Heatstroke: a multicenter study in Southwestern China.Front Public Health. 2024 Apr 17;12:1349753. doi: 10.3389/fpubh.2024.1349753. eCollection 2024. Front Public Health. 2024. PMID: 38699425 Free PMC article.
-
A NOMOGRAM FOR PREDICTING PATIENTS WITH SEVERE HEATSTROKE.Shock. 2022 Aug 1;58(2):95-102. doi: 10.1097/SHK.0000000000001962. Epub 2022 Jul 24. Shock. 2022. PMID: 35953457
-
[A multicenter clinical study of critically ill patients with sepsis complicated with acute kidney injury in Beijing: incidence, clinical characteristics and outcomes].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024 Jun;36(6):567-573. doi: 10.3760/cma.j.cn121430-20240210-00124. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024. PMID: 38991953 Chinese.
-
[Analysis of risk factors of prolonged intensive care unit stay of critically ill obstetric patients: a 5-year retrospective review in 3 hospitals in Beijing].Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2011 Aug;23(8):449-53. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2011. PMID: 21878165 Chinese.
-
Gastrointestinal manifestations of critical ill heatstroke patients and their associations with outcomes: A multicentre, retrospective, observational study.World J Gastroenterol. 2024 Jan 28;30(4):346-366. doi: 10.3748/wjg.v30.i4.346. World J Gastroenterol. 2024. PMID: 38313238 Free PMC article.
References
-
- Vose R.S., Easterling D.R., Kunkel K.E., LeGrande A.N., Wehner M.F. 2017: Temperature changes in the United States. In: Climate Science Special Report: Fourth National Climate Assessment, Volume I, 2017(4).
MeSH terms
LinkOut - more resources
Full Text Sources
