

COMPOSIT study: evaluating osimertinib combination with targeted therapies in EGFR-mutated non-small cell lung cancer
- PMID: 39724403
- PMCID: PMC12395140
- DOI: 10.1093/oncolo/oyae312
COMPOSIT study: evaluating osimertinib combination with targeted therapies in EGFR-mutated non-small cell lung cancer
Abstract
Introduction: The emergence of diverse resistance mechanisms after osimertinib therapy, including on-target epidermal growth factor receptor (EGFR) mutations and off-target alterations, warrants investigation of novel therapeutics to overcome these challenges and improve patient outcomes.
Methods: COMPOSIT was a French, retrospective, multicenter, cohort study of the effectiveness and tolerability of osimertinib in combination with other targeted therapies in patients with advanced EGFR-mutant (EGFRm) non-small cell lung cancer (NSCLC) who harbored other oncogenic drivers as primary or acquired resistance mechanisms. Real-world progression-free survival (rwPFS), overall survival (OS), and objective response rate (ORR) were the primary endpoints.
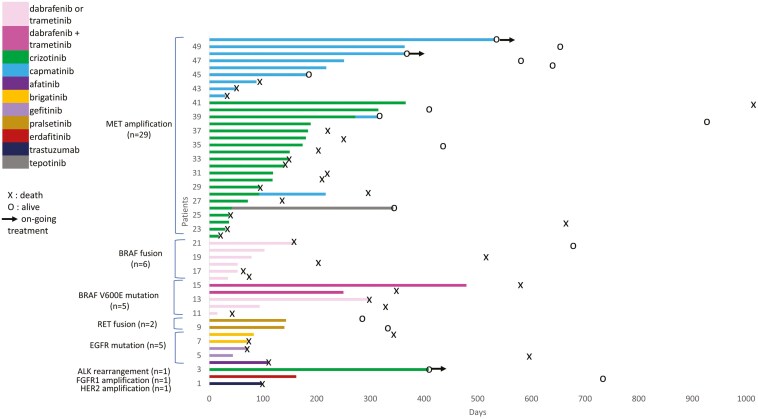
Results: The study included 61 patients (63.9% women; median age, 61 years). Chemotherapy was administered to 26 patients (42.6%) before the combinations. The most frequently targeted resistance mechanisms were MET amplification (n = 40) and BRAF alterations (n = 11). Sixteen combinations of osimertinib with other targeted therapies were reported. Overall (except for 10 patients in clinical trials), median rwPFS and OS were 3.9 (95% CI, 2.9-5.2) and 9.8 months (95% CI, 6.8-14.8). Best ORR (n = 54) was 50% (95% CI, 33.0-72.8). In patients with MET amplification (n = 29), median rwPFS and OS were 4.9 (95% CI, 2.9-7.2) and 8.6 months (95% CI, 5.3-21.6). Grade ≥3 adverse events occurred in 15 patients (24.6%). No deaths were related to treatment.
Conclusions: Combinations of osimertinib with other targeted therapies appeared to be feasible and safe and may offer clinical benefit to overcome resistance to osimertinib in EGFRm NSCLC, especially in patients with MET amplification.
Keywords: EGFR TKI resistance; EGFR mutation; combinations; non-small cell lung cancer; osimertinib; real-world study.
© The Author(s) 2024. Published by Oxford University Press.
Conflict of interest statement
A.S. has received personal consulting fees, honoraria for presentations, speakers bureaus, or educational events, and personal support for attending meetings participation from Amgen, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo Inc., F. Hoffman La Roche, Ipsen, Jansen, Lilly, MSD, Novartis, Pfizer, Sanofi and Takeda. I.M. has received personal support for attending meetings participation from Pfizer, Takeda, Sanofi, Astra Zeneca. M.W. has received personal consulting fees and personal support for attending meetings participation from Amgen, Astra Zeneca, BMS, Janssen, Lilly, Merck Serono, Novartis, Pfizer, Roche, Takeda. F.G. has received personal fees for consulting or lectures from Amgen, Astra Zeneca, BMS, Sanofi, Viatris, Takeda, Roche, MSD, Pfizer, and Janssen, and research grants to institutions from Takeda, Roche, and Pfizer, outside of the submitted work. H.C. has received consulting fees or honoraria from BMS and registration fees and accommodations from Sandoz. P.D.R. has received personal consulting fees and personal support for attending meetings participation from Amgen, Astra Zeneca, BMS, Daiichi Sankyo, Eisai, Janssen, Lilly, Merck Serono, Mundipharma, Novartis, Pfizer, Roche, Sandoz, Sanofi and Takeda. A.B.C. had received research grants (paid to institution) from Merck, consulting fees from Novartis and Roche, a speaker honorarium from Astra-Zeneca, BMS, MSD, Pfizer, Novartis, Takeda, Janssen, Roche, Abbvie, Amgen and Exeliom and support from Pfizer, Novartis and MSD to attend meetings and had served on advisory boards from Novartis and InhaTarget. V.G. has received personal fees from Astra, BMS; personal fees, and non-financial support from Janssen, Sanofi, Takeda, Pfizer, Roche; all outside the submitted work. B.A. has received consulting fees or honoraria from Novartis, AstraZeneca, BMS, MSD, Astellas, and Sanofi. E.G.L. has received personal consulting fees, honoraria for presentations, speakers bureaus, and personal support for attending meetings participation from Amgen, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, F. Hoffman La Roche, Janssen, Lilly, MSD, Novartis, Pfizer, Sanofi and Takeda. T.P. has received personal consulting fees, honoraria for presentations, and personal support for attending meetings participation from BMS, Pfizer, Takeda, Sanofi, Janssen, and MSD. B.D. has received grants, travel, and honoraris from Roche, Pfizer, Astra Zeneca, Chiesi, Amgen, Lilly, Medscape, MSD, Sanofi, and Oxyvie. F.M.Q. has received personal consulting fees and personal support for attending meetings participation from Astra Zeneca, BMS, and Pfizer. J.C. has received personal consulting fees, honoraria for presentations, speakers bureaus, or educational events, and personal support for attending meetings participation from Amgen, AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo Inc, F. Hoffman La Roche, Janssen, Lilly, MSD, Novartis, Pfizer, Sanofi and Takeda. V.F. has received personal consulting fees, honoraria for presentations, speakers bureaus, or educational events, and personal support for attending meetings participation from Amgen, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, F. Hoffman La Roche, Jansen, MSD Oncology, Novartis, Pfizer, Sanofi, and Takeda. All remaining authors have declared no conflicts of interest. The authors declare that they have no known competing financial interests or personal relationships that could influence the work reported in this article.
Figures


References
-
- Barlesi F, Mazieres J, Merlio J-P, et al. ; Biomarkers France contributors. Routine molecular profiling of patients with advanced non-small-cell lung cancer: results of a 1-year nationwide programme of the French Cooperative Thoracic Intergroup (IFCT). Lancet (London, England). 2016;387:1415-1426. https://doi.org/ 10.1016/S0140-6736(16)00004-0 - DOI - PubMed
-
- Ramalingam SS, Vansteenkiste J, Planchard D, et al. ; FLAURA Investigators. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382:41-50. https://doi.org/ 10.1056/NEJMoa1913662 - DOI - PubMed
-
- Passaro A, Leighl N, Blackhall F, et al. ESMO expert consensus statements on the management of EGFR mutant non-small-cell lung cancer. Ann Oncol. 2022;33:466-487. https://doi.org/ 10.1016/j.annonc.2022.02.003 - DOI - PubMed
-
- Yang JC-H, Ahn M-J, Kim D-W, et al. Osimertinib in pretreated T790M-positive advanced non–small-cell lung cancer: AURA study phase II extension component. J Clin Oncol. 2017;35:1288-1296. https://doi.org/ 10.1200/JCO.2016.70.3223 - DOI - PubMed
-
- Oxnard GR, Hu Y, Mileham KF, et al. Assessment of resistance mechanisms and clinical implications in patients with EGFR T790M-positive lung cancer and acquired resistance to osimertinib. JAMA Oncol. 2018;4:1527. https://doi.org/ 10.1001/jamaoncol.2018.2969 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
